Implant Breast Reconstruction
For women who choose implant reconstruction, this typically entails multiple stages. Initially, tissue expanders are placed underneath the muscles of the chest at the time of mastectomy. The patient then undergoes sequential inflations of the expander using saline to create a sizable ‘pocket’ for the subsequent implant. Dr. Haddock usually is able to expand his patients significantly at the time of the mastectomy. This provides the benefit of providing some initial breast shape and volume while also limiting the postoperative expansion visits for his patients. These expansion procedures occur in Dr. Haddock's office. Once the appropriate ‘pocket’ has been achieved, the patient returns to the operating room for removal of the tissue expander in exchange for a silicone or saline implant. Both types are available, and to date, no study has documented a cause and effect relationship between silicone or saline implants and systemic illness.
Recently, there has been a movement to reduce the number of procedures needed for implant reconstruction by eliminating the need for tissue expansion. In some unique situations a direct to implant route is an option. This is only available in the ideal situation and if this scenario exist will be discussed in consult with Dr. Haddock.
Regardless of whether a tissue expander is used or not, the principle benefit of using implants for breast reconstruction is that it provides a method of reconstruction that is relatively straightforward and can limit the surgical site to the breast. Aesthetically, Dr. Haddock can create a youthful, aesthetically appealing breast with either shaped or round implants. Implant reconstruction does, however, have functional downsides. The implant can be palpable and/or visible through the breast skin. The degree of palpability and visibility is dependent on the thickness of the mastectomy flaps. Regardless an implant reconstruction is always less natural in shape and consistency when compared to a natural breast.
Dr. Haddock does routinely offer fat grafting to his patients. This involves liposuction of an area of unwanted fat, processing this fat to remove any extra tissue, and then injecting the fat around the implant to provide an optimal aesthetic result and more natural feeling. Dr. Haddock typically will offer this at the time of implant exchange and at the time of nipple reconstruction.
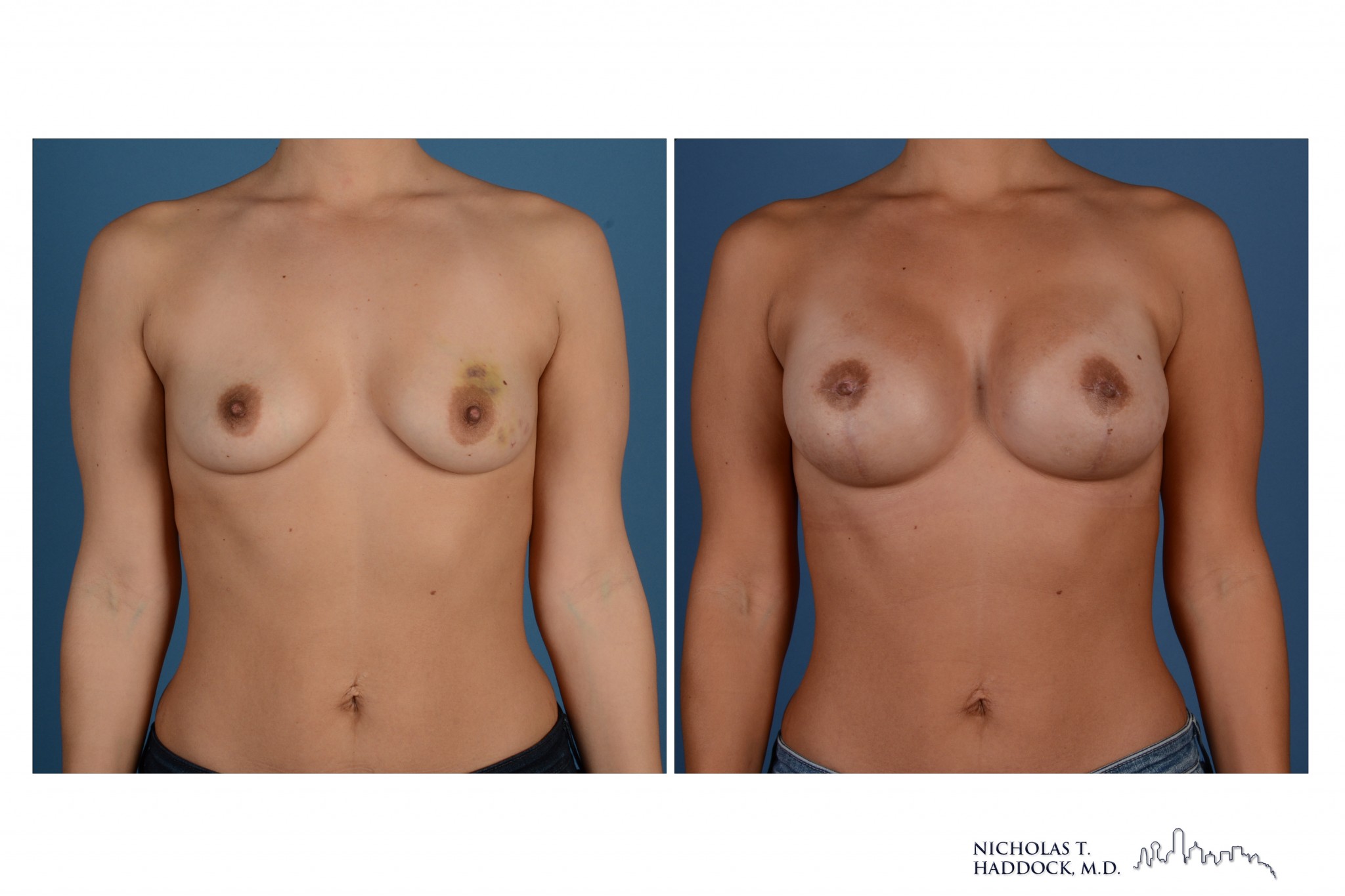
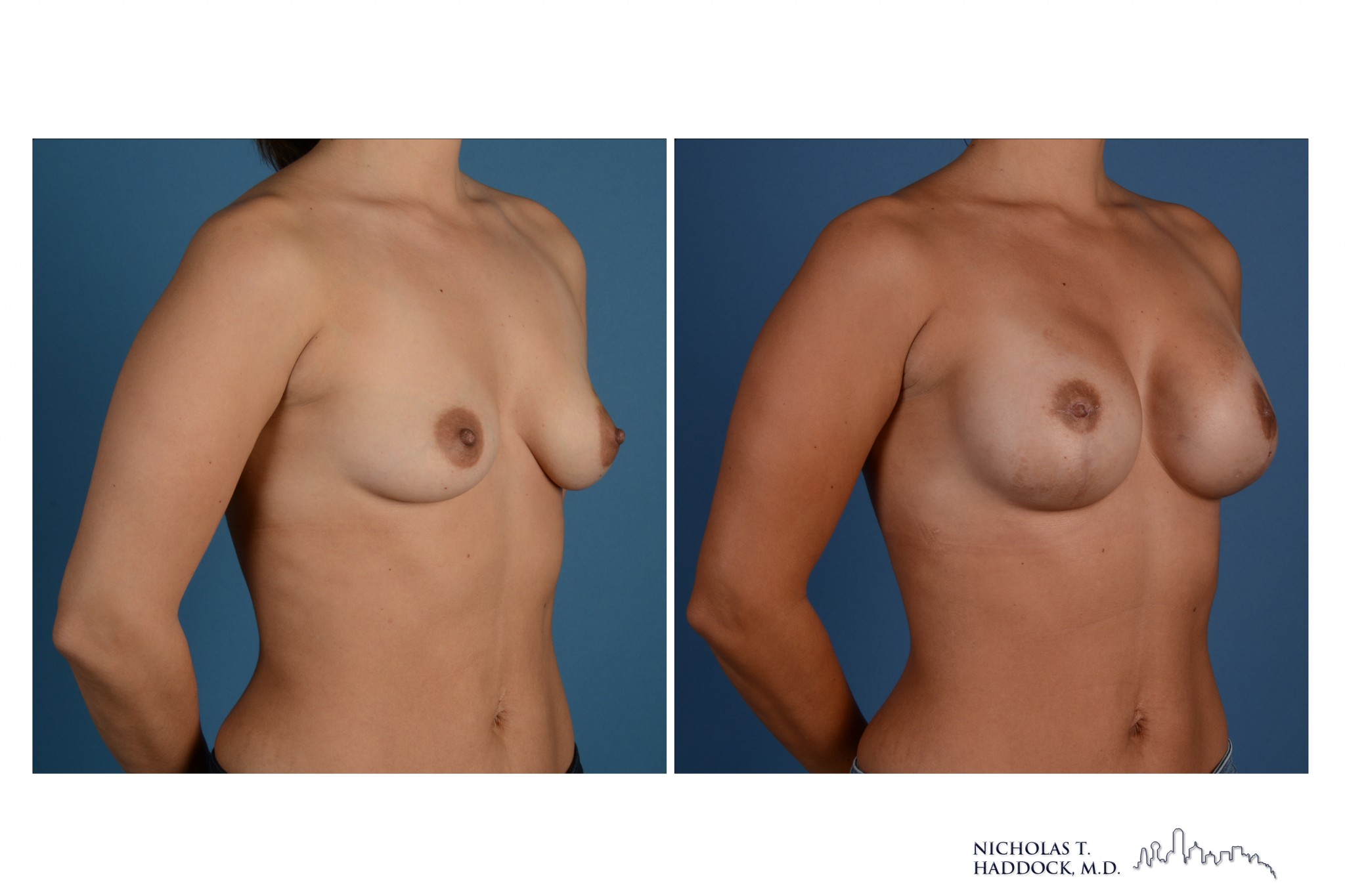
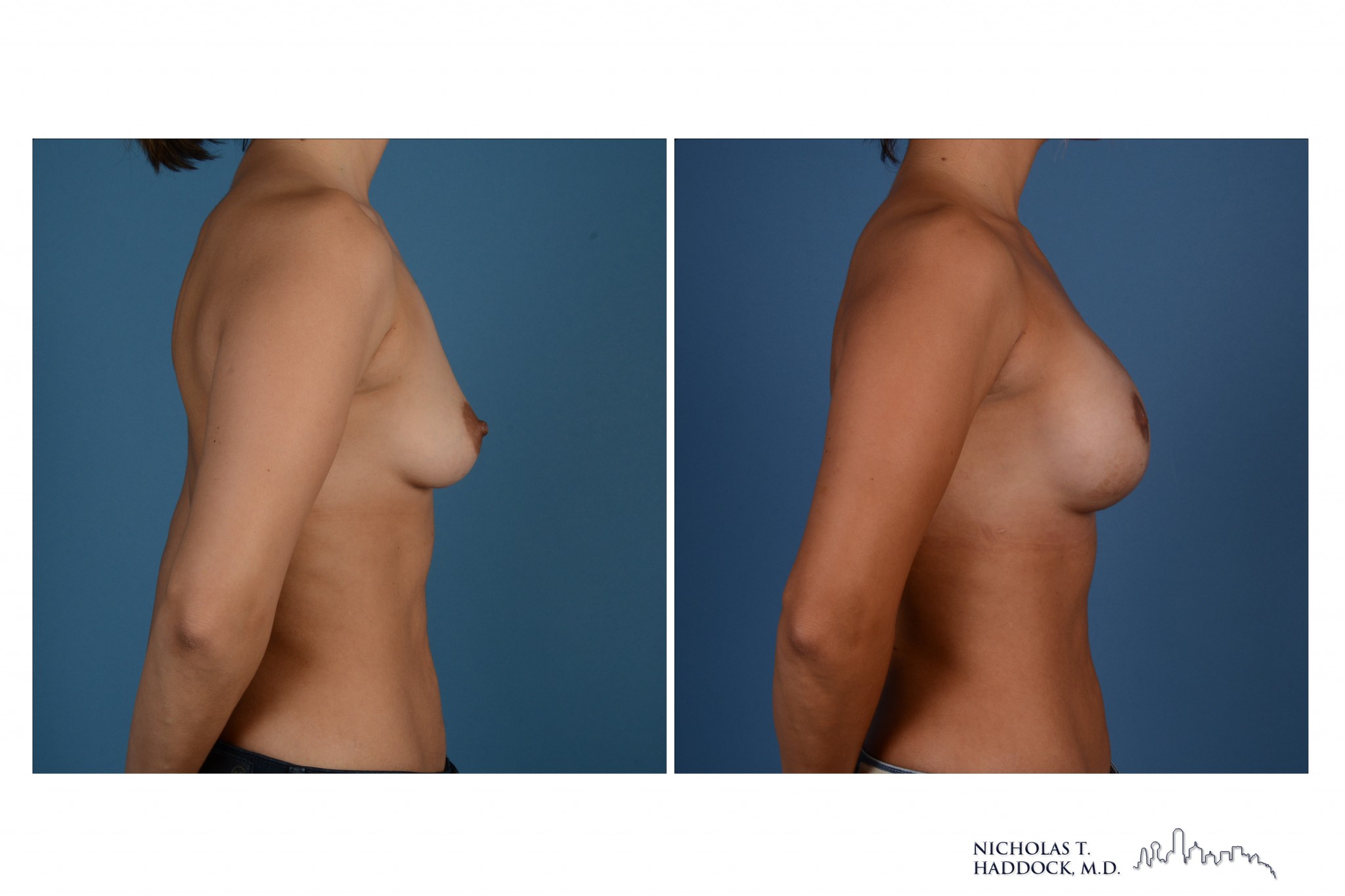
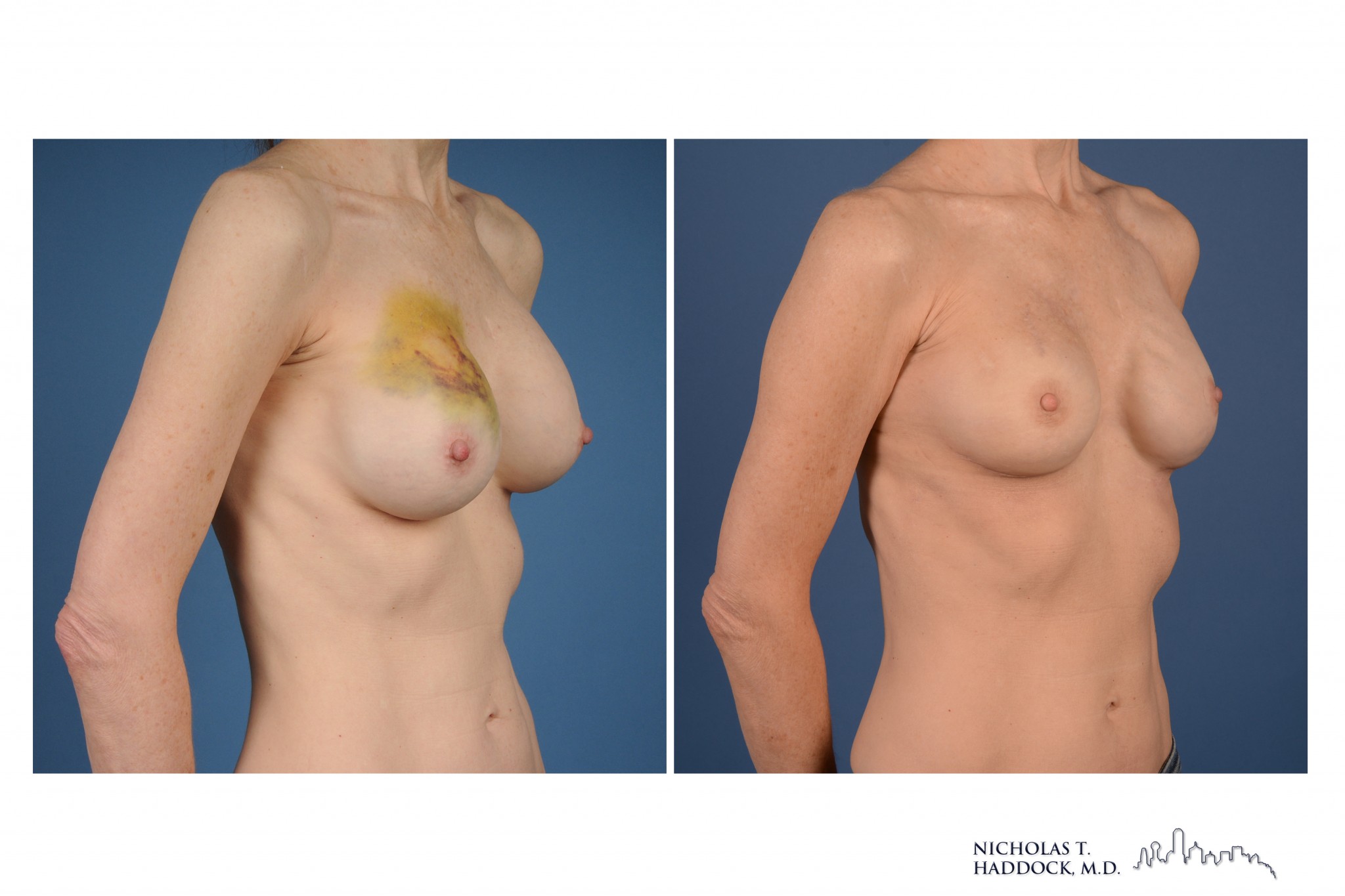
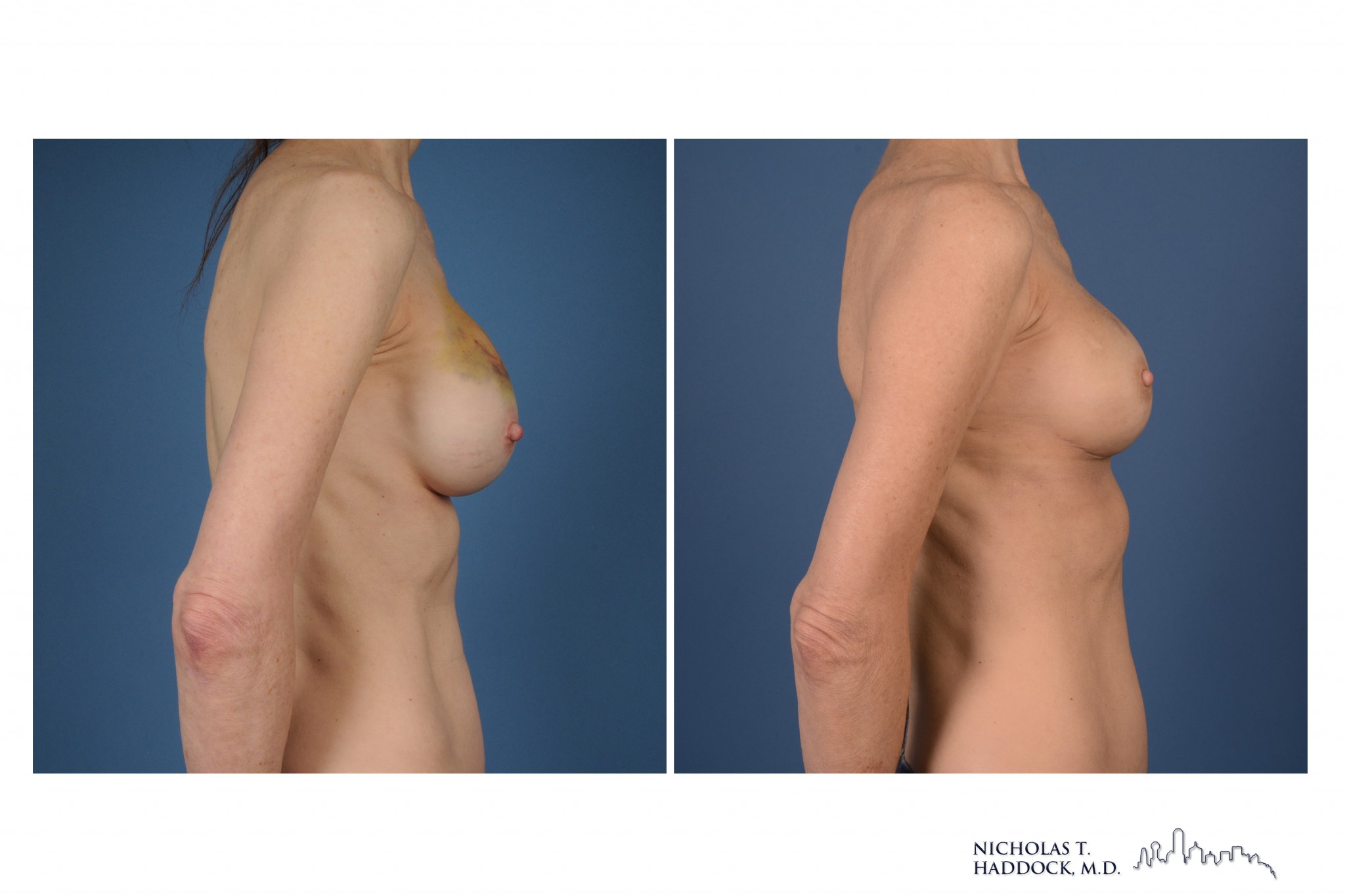
Bilateral mastectomies followed by reconstruction with shaped implants and nipple reconstruction
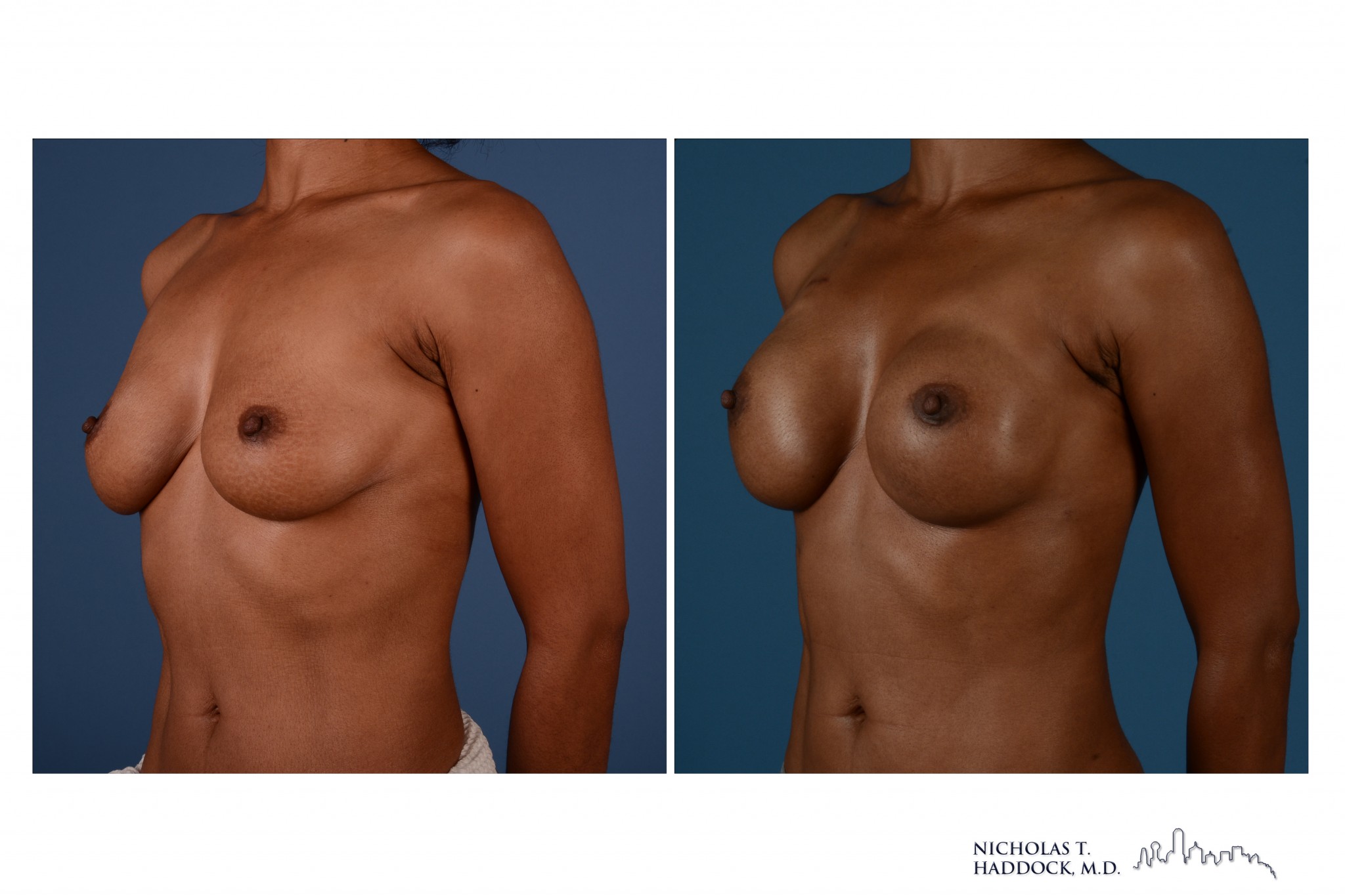
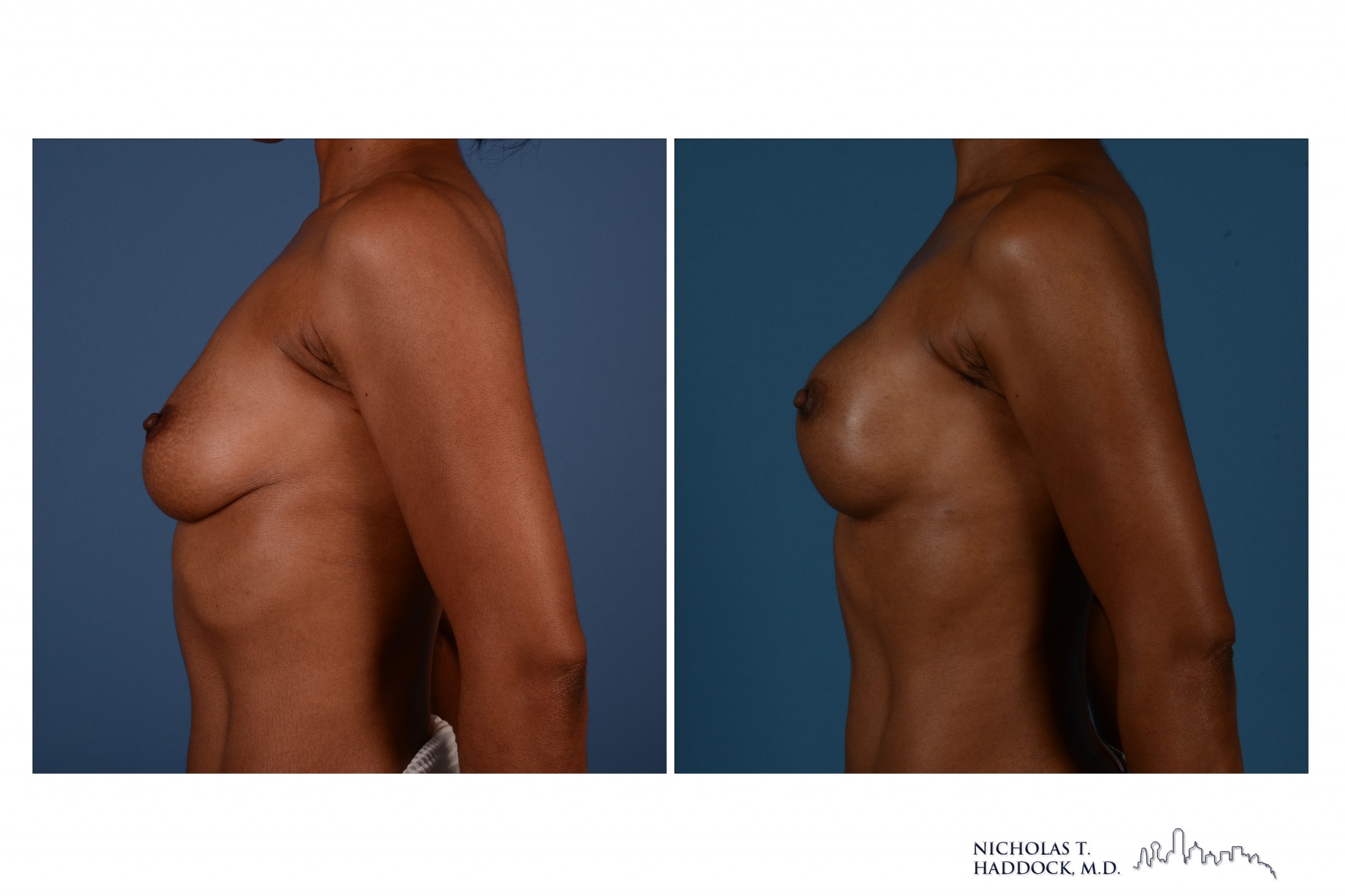
Bilateral nipple sparing mastectomies followed by immediate reconstruction with round implants (1 surgery)

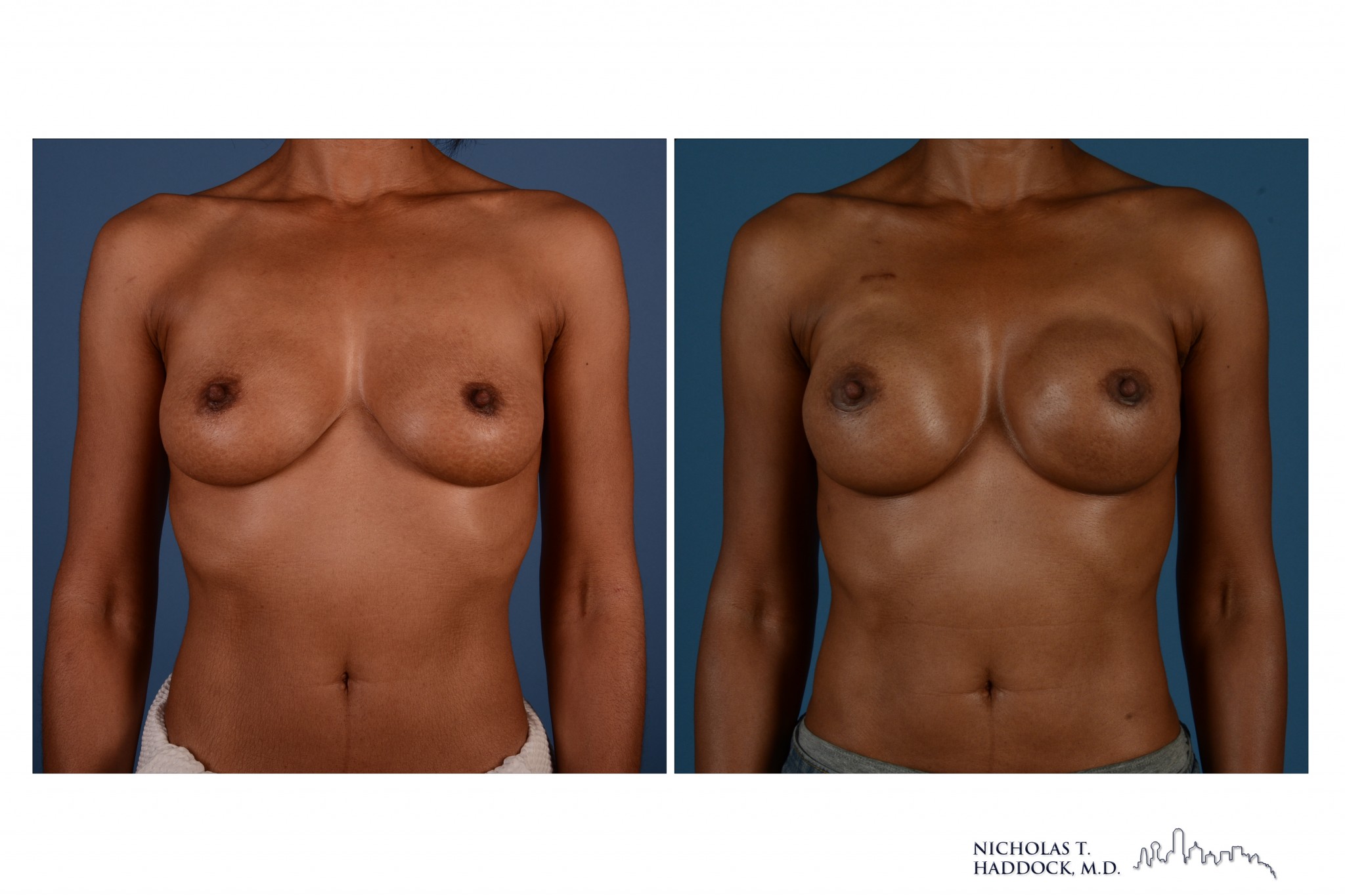
Bilateral mastectomies followed by reconstruction with round implants and nipple reconstruction
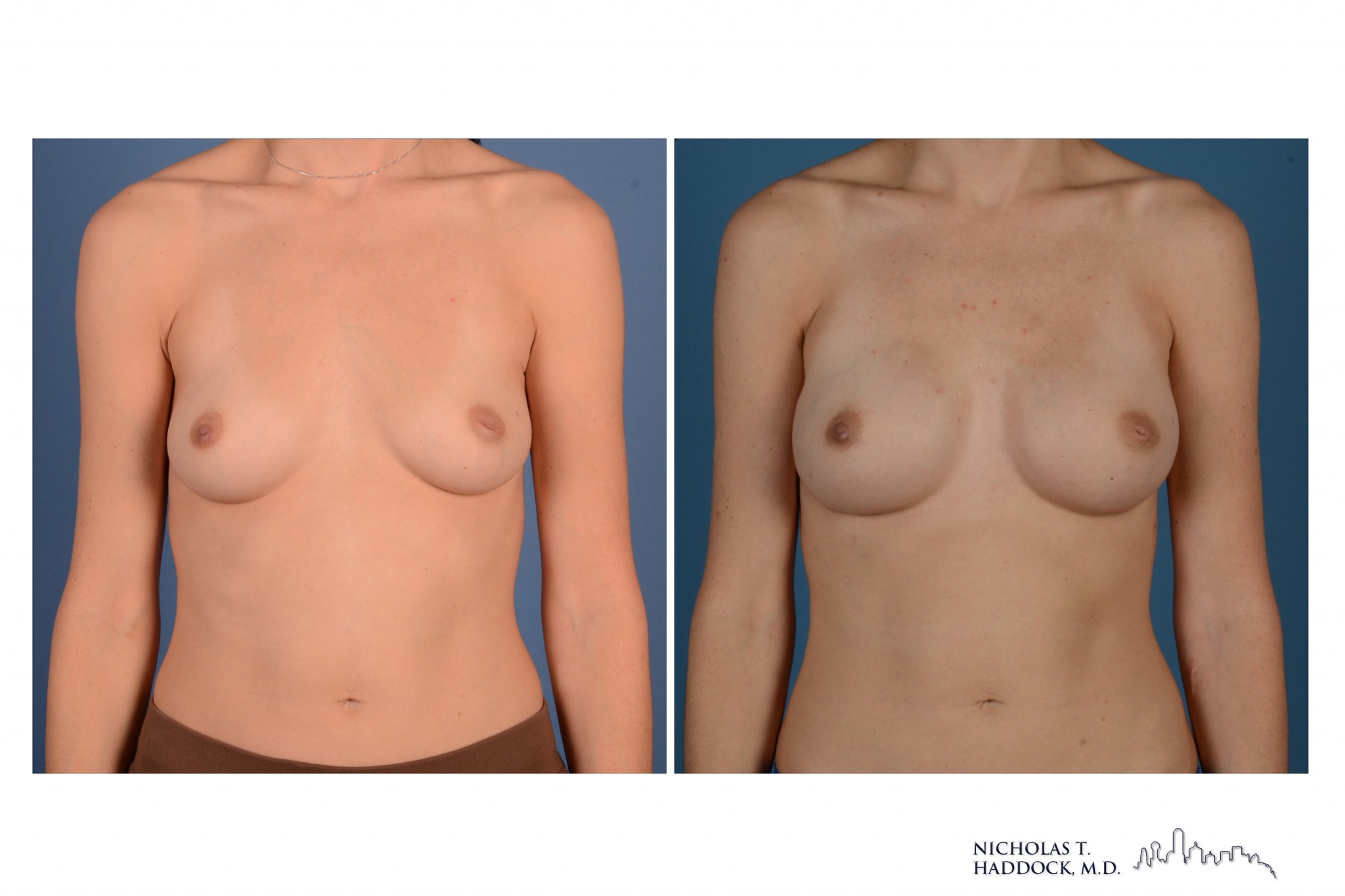
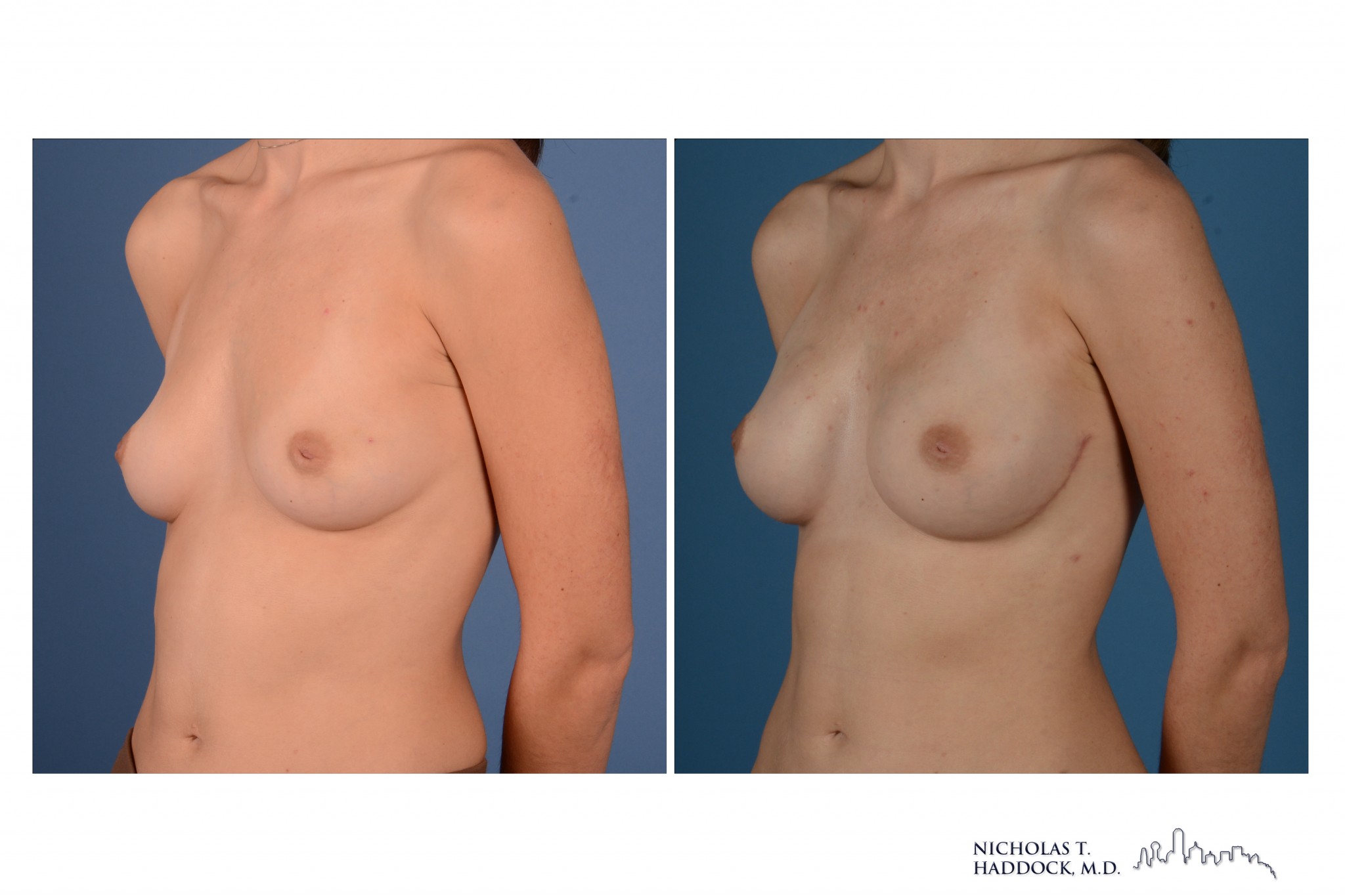
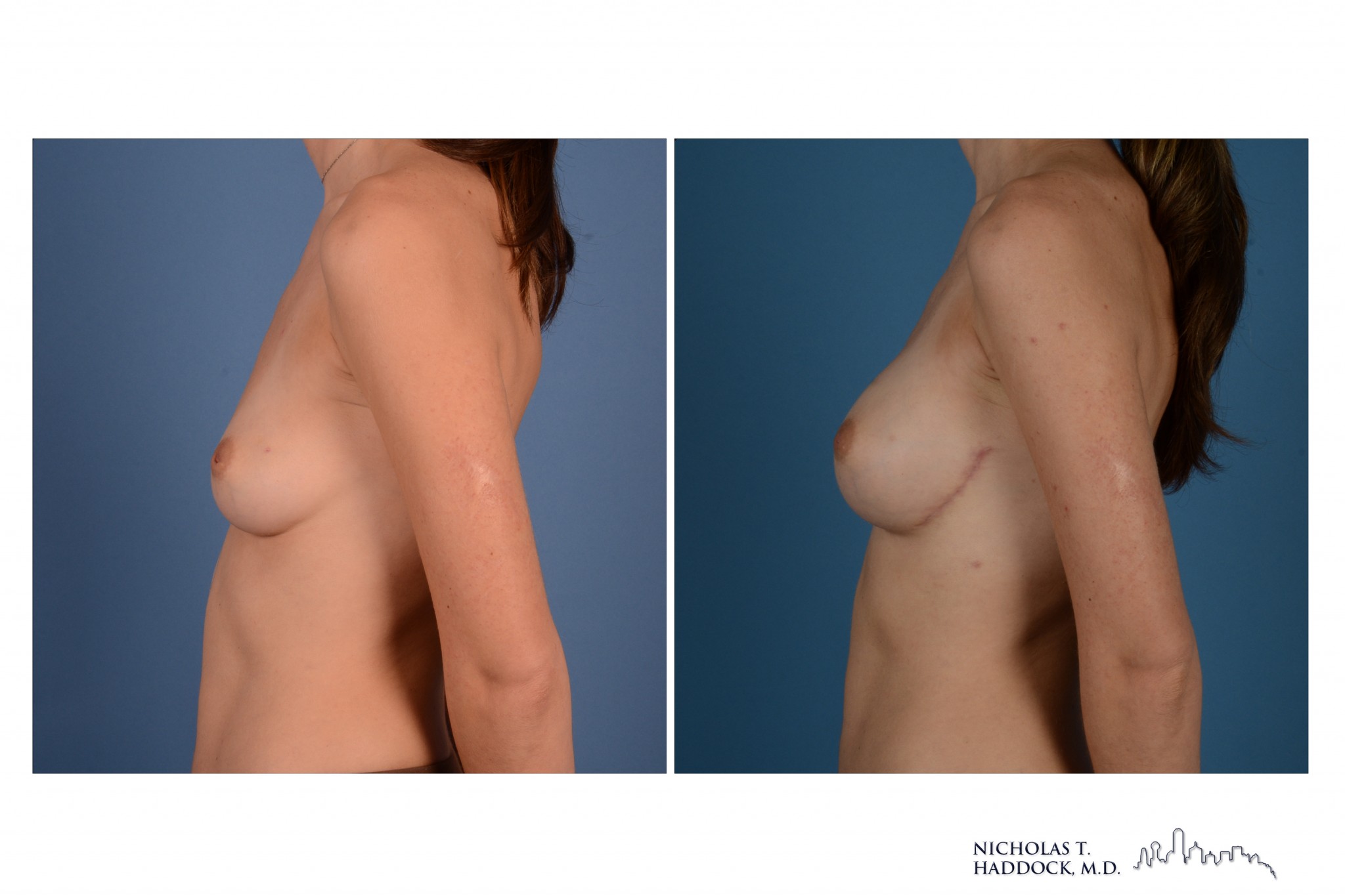
Bilateral nipple sparing mastectomies followed by reconstruction with shaped implants
Latissimus Dorsi Flap with an Implant
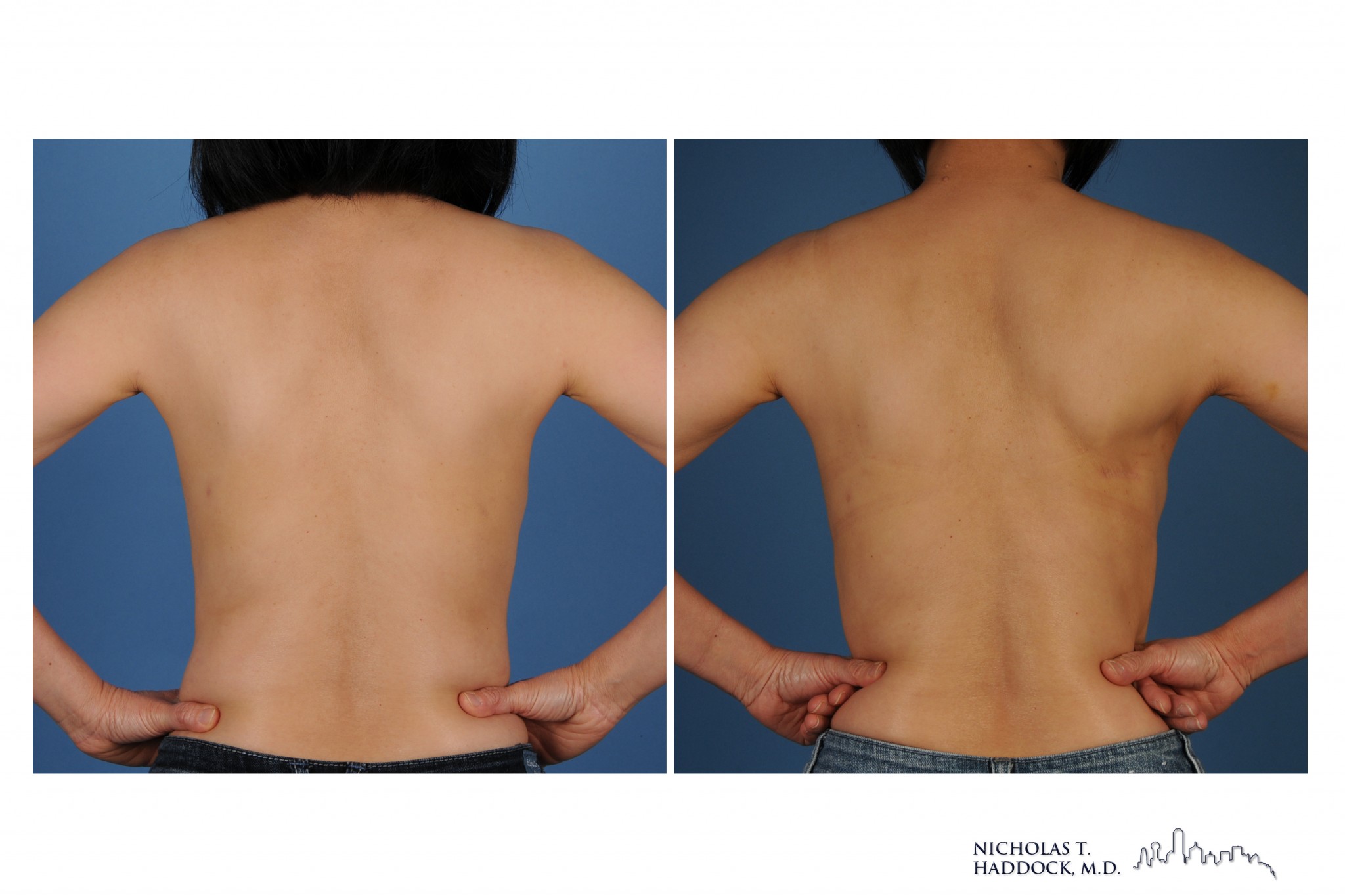
The latissimus dorsi flap provides skin, fat, muscle from the back that can be pedicled to the breast. This flap can be rotated directly from the back to the breast and therefore there is no microsurgery involved in this flap as there is in some other options. The main draw back of this flap is that in most people it does not provide enough bulk to reconstruct a moderate sized breast. In these situations often a tissue expander or implant is required. In specific situations Dr. Haddock can offer a minimally invasive latissimus flap with an incision that is only a few centimeters in length. Additionally, for partial breast reconstruction Dr. Haddock can perform a muscle sparing latissimus flap or a thoracodorsal artery perforator (TDAP) flap.
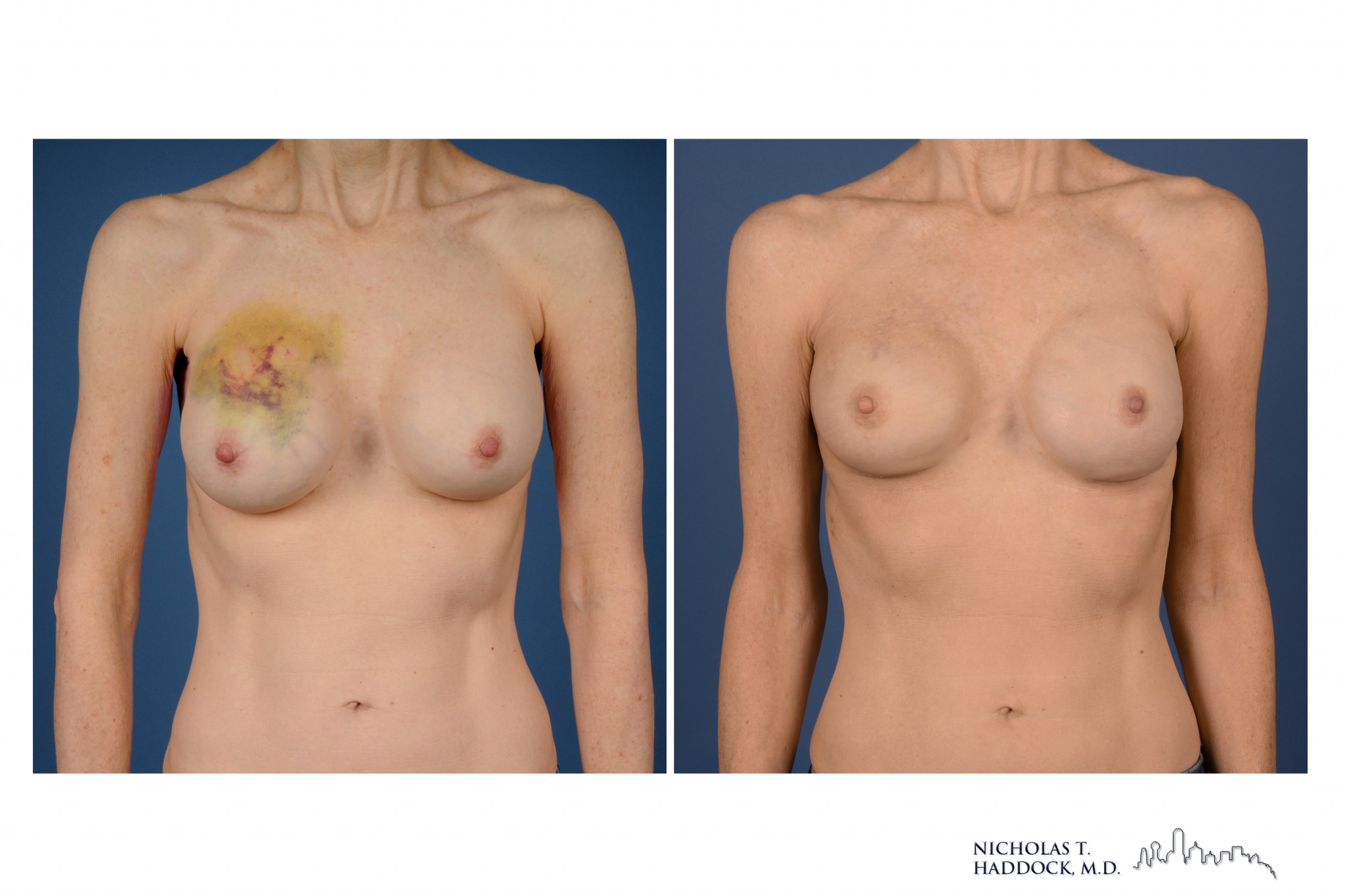

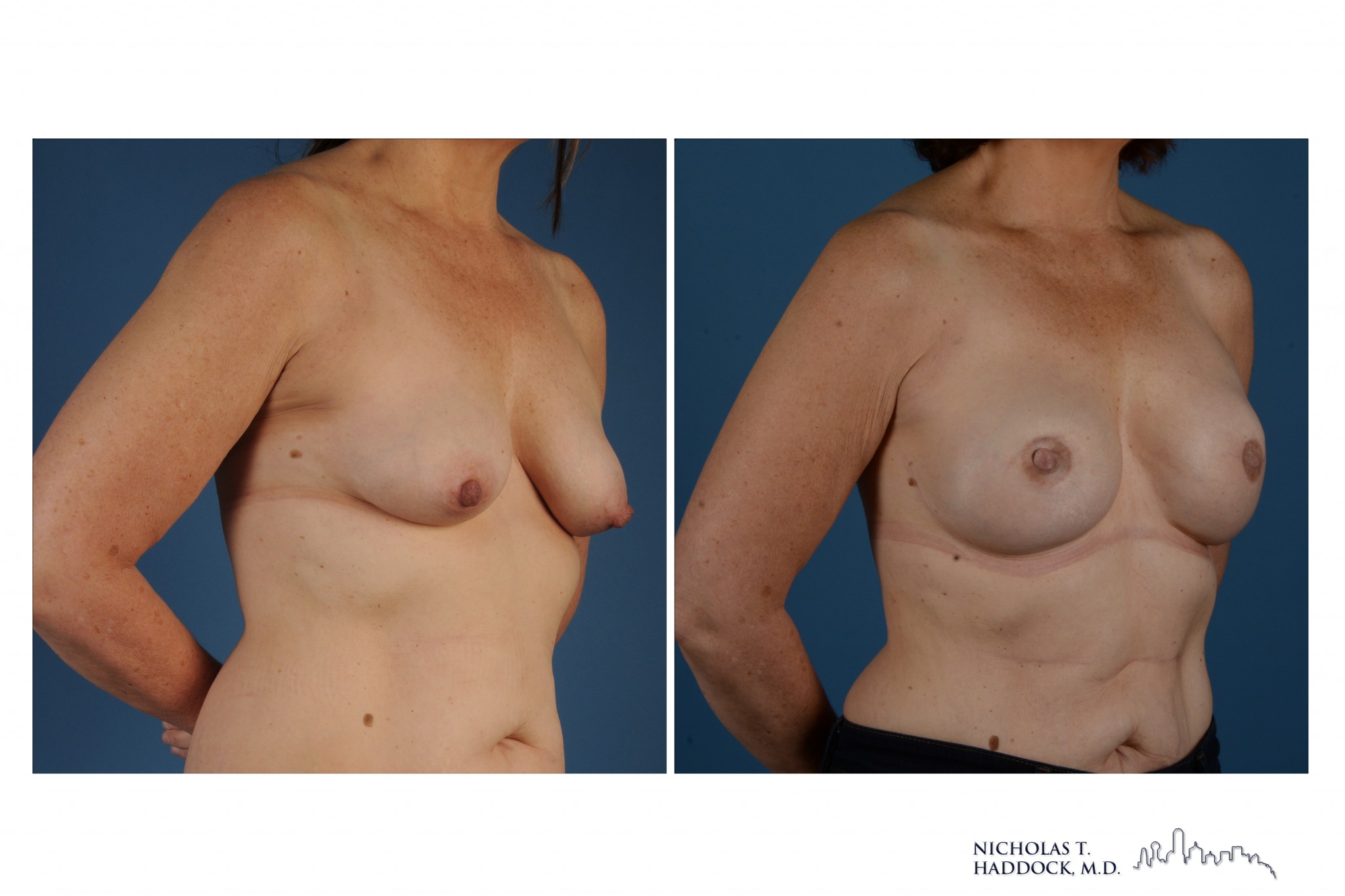
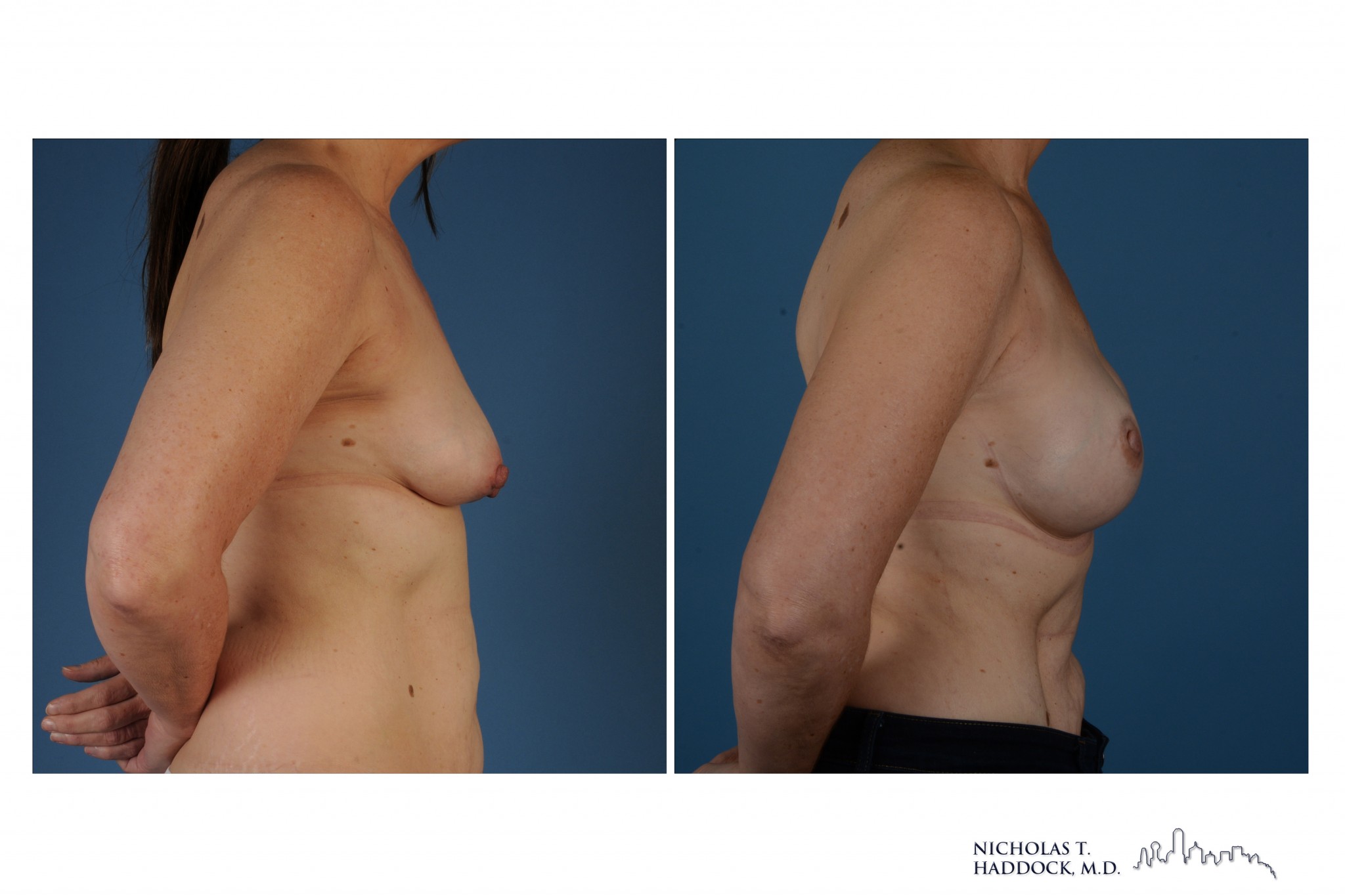
Bilateral nipple sparing mastectomies with right radiation
Right latissimus muscle flap and bilateral implants
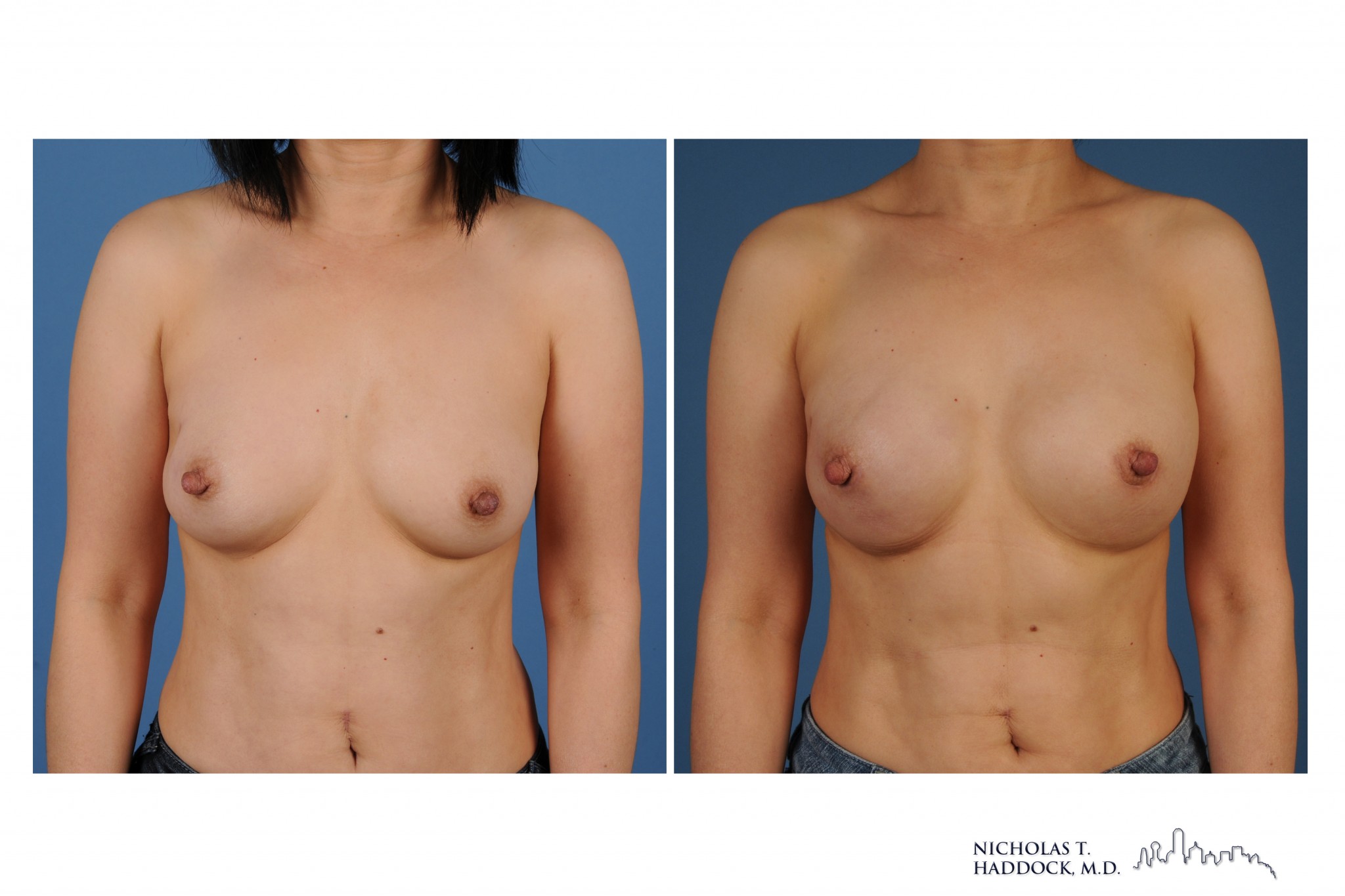

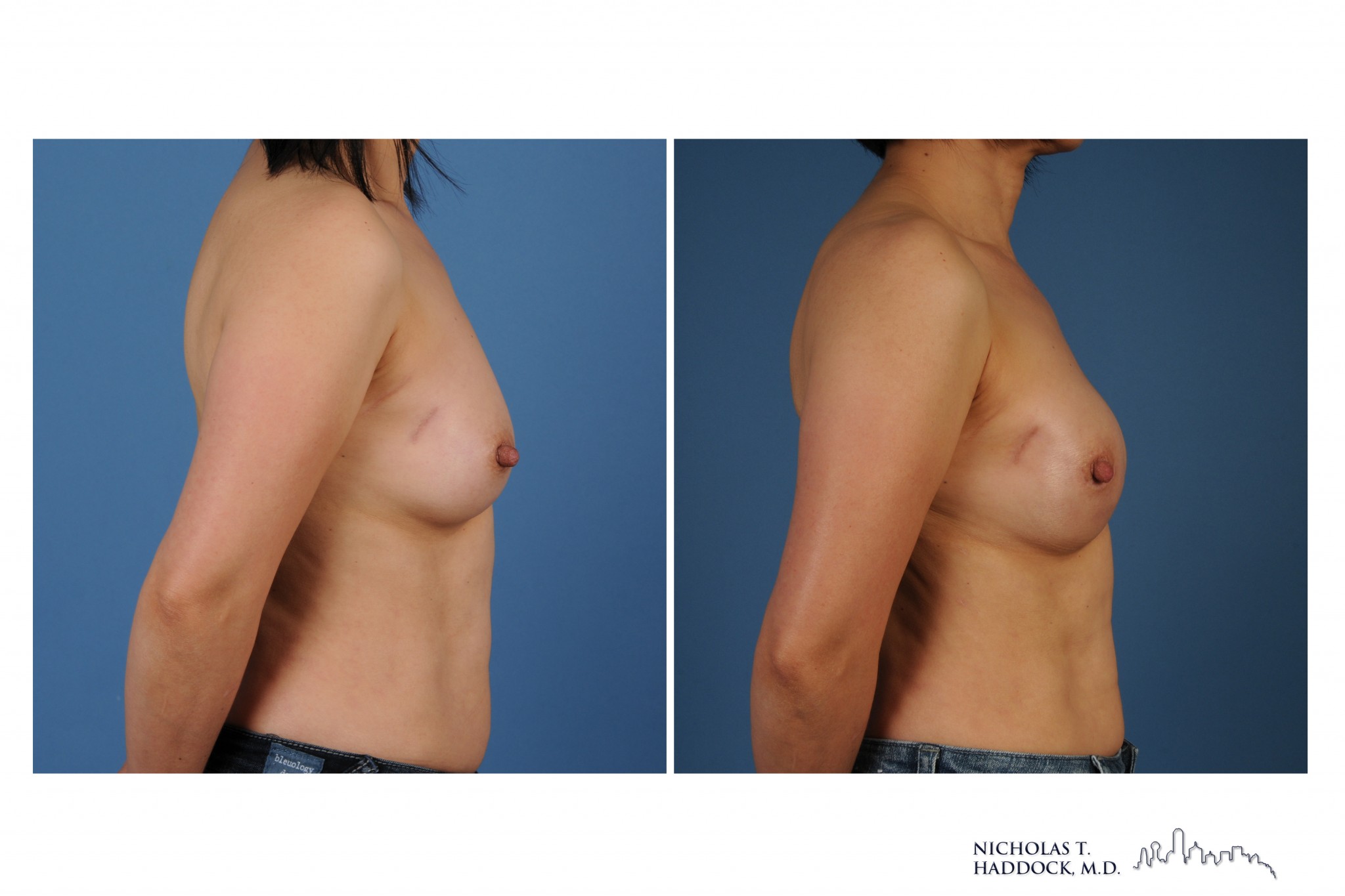
Bilateral nipple sparing mastectomies with right radiation
Right latissimus muscle flap and bilateral implants
Risks/Potential Complications Associated With Implant Based Reconstruction
Implants carry the risk of infection, the most common perioperative implant related complication. A further potential complication associated with implant reconstruction is capsular contracture. This is caused by an abnormal immunological response to foreign bodies and occurs when the capsule that forms around the breast implant tightens and squeezes the implant. In rare cases it can be painful and translates to a firming of the breast and a deformation of the reconstruction. Severe contractures, also known as Baker grade III or IV contractures, occur in a small percentage of patients. Finally, implants will rupture at rates of approximately 1% per year, regardless of whether saline or silicone implants are used. Implants are not lifelong devices, and the patient will likely need one or more procedures to replace the implant over her lifetime.
To schedule a breast reconstruction consultation with Dr. Haddock, please contact us.
