Flap Breast Reconstruction
DIEP Flap and PAP Flap
Flap Success Rate
Flap Success Rate

The most common donor location of autologous tissue breast reconstruction is the lower abdomen. This tissue can be transferred as a pedicled flap based on the superior epigastric vessels, or as a free flap based on the deep inferior epigastric vessels (DIEP flap) or superficial inferior epigastric vessels (SIEA flap). Pedicled flaps remain connected to their native arterial and venous supply, while the tissue is transferred to the new location. Free flaps are completely disconnected from their original blood supply and a new connection is subsequently performed in the new location. From our experience it is clear that free flaps are a better option for nearly all patients. The secondary location for tissue is the back of the thigh (PAP flap).
Patients desiring autologous tissue reconstruction from the abdomen must have sufficient lower abdominal tissue available to reconstruct the breast. If such tissue is present, there are very few contraindications that preclude a patient from having this type of reconstruction. If the lower abdomen is not a sufficient donor site, or if previous surgery eliminates the potential use of this tissue, a number of alternative flaps from other parts of the body have been developed as additional options. Dr. Haddock was a pioneer in the PAP flap (posterior thigh) and this is his first choice as a second option to the abdomen.
Choosing Your Plastic Surgeon
Dr. Haddock is an expert at the deep inferior epigastric perforator flap (DIEP). He has performed hundreds of these with routinely very high success rates. His approach is focused on a few key goals including superior aesthetic results, limited abdominal morbidity, and operative efficiency leading to quick recovery. When choosing a surgeon to perform this operation experience is key. Additionally, the focus of the operation can vary among surgeons. Dr. Haddock does not simply view success as flap survival but his goal is to achieve the result his patients want.
As in all procedures, there are complications associated with autologous breast reconstruction. The potential adverse outcomes of autologous tissue breast reconstruction are total flap failure or partial flap failure. Total flap failure, the most feared complication, typically occurs due to a venous or arterial thrombosis of the vessels supplying the flap. With improved operative technique, in experienced hands this risk is extremely low. If the tissue is taken from the abdomen, it is possible that problems with abdominal weakness, hernia, or bulge may occur. The chance of occurrence of abdominal weakness and hernia or bulge vary according to the different type of flap used. Dr. Haddock works very hard to avoid damage to the abdominal muscles to avoid these potential adverse outcomes. Patients may also experience hematomas, seromas and wound healing problems at the donor site or the recipient site.
DIEP Flap

The Deep Inferior Epigastric Perforator (DIEP) flap replaces the skin and soft tissue removed at mastectomy with tissue that is borrowed from the abdomen. A slim incision along the bikini line is made, much like that used for a tummy tuck. The skin, soft tissue, and very small blood vessels required to produce the breast reconstruction are removed from the abdomen. These small blood vessels are matched to supplying vessels at the mastectomy site and reattached under a microscope. Unlike conventional TRAM (Transverse Rectus Abdominis Muscle) flap reconstructions, the use of the perforator flap technique allows the collection of the required tissue without sacrifice the underlying abdominal muscles. This tissue is then surgically transformed into a new breast mound. The abdomen is a favorable donor site for many woman, since excess fat and skin are often found in this area. In addition to reconstructing the breast, the contour of the abdomen is often improved, much like a tummy tuck.
Like the DIEP, the Superficial Inferior Epigastric Artery (SIEA) flap replaces the skin and soft tissue removed at mastectomy with tissue from the abdomen. In a select group of women the blood vessels just under the skin are used as feeding vessels for the abdominal skin and fat. The use of these superficial vessels allows the surgeon to completely avoid the abdominal muscles because the blood vessel used do not travel within the muscle. The vessel supplying the lower abdominal tissue are preserved and the transferred skin and fat are transformed into a new breast mound. The procedure is otherwise the same as the DIEP flap, resulting in a low abdominal incision much like a tummy tuck.
The Transverse Rectus Abdominis (TRAM) Flap is similar in design to both the DIEP and the SIEA flaps. In contrast to the other two flaps, in some situations a portion of the rectus muscle must be taken with the abdominal skin and fat. The decision to remove some muscle is based solely on the anatomy of the patient. Preoperative imaging helps to determine if this will be required, but ultimately the decision is often made in the operating room. The TRAM flap offers similar results in the breast but does sacrifice some muscle to obtain that result. In Dr. Haddock’s practice it is very rare that he has to use a TRAM flap as he almost always can use a DIEP or SIEA flap. If a TRAM is used then the abdominal contour is still similar to a tummy tuck.
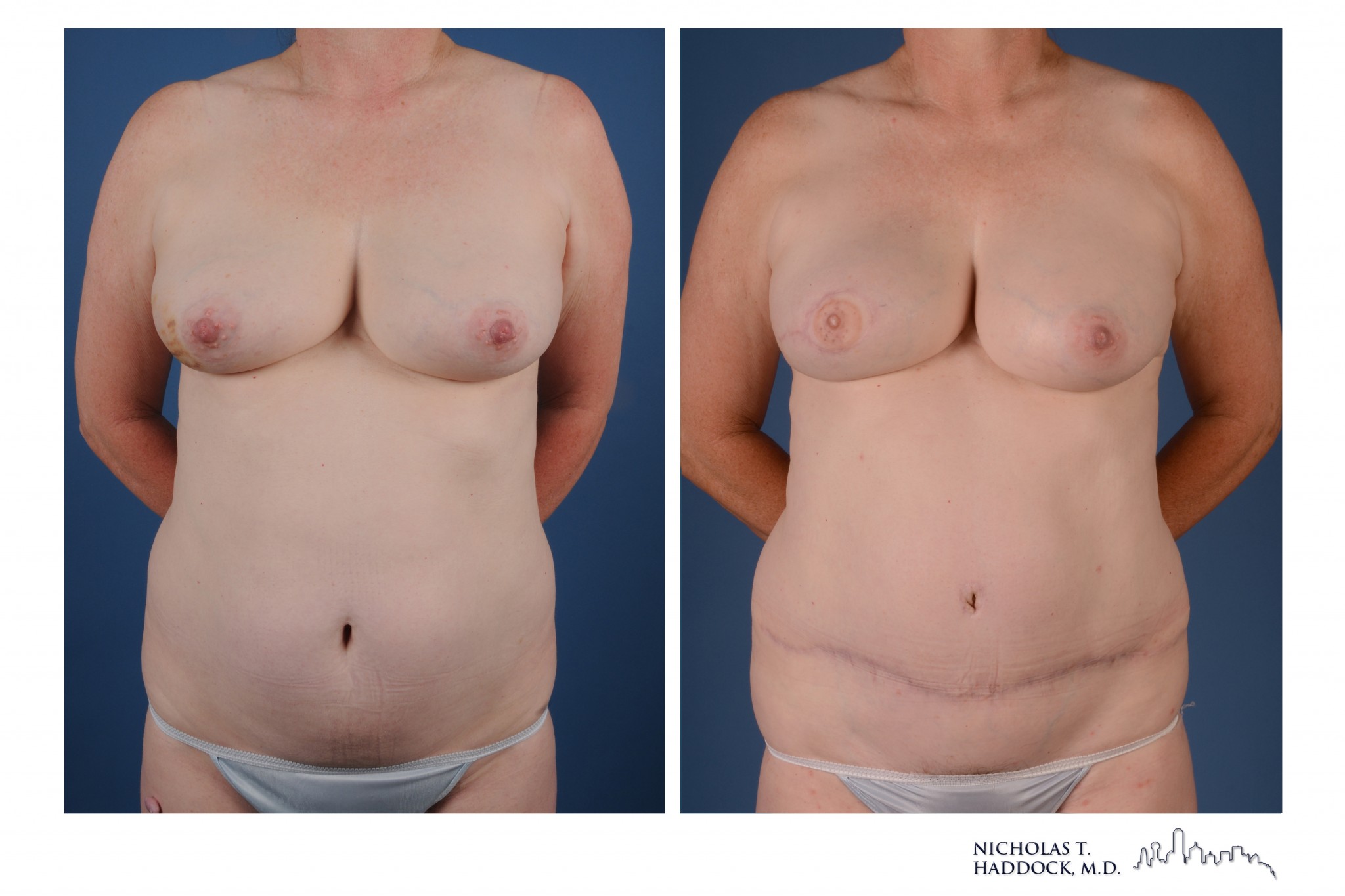
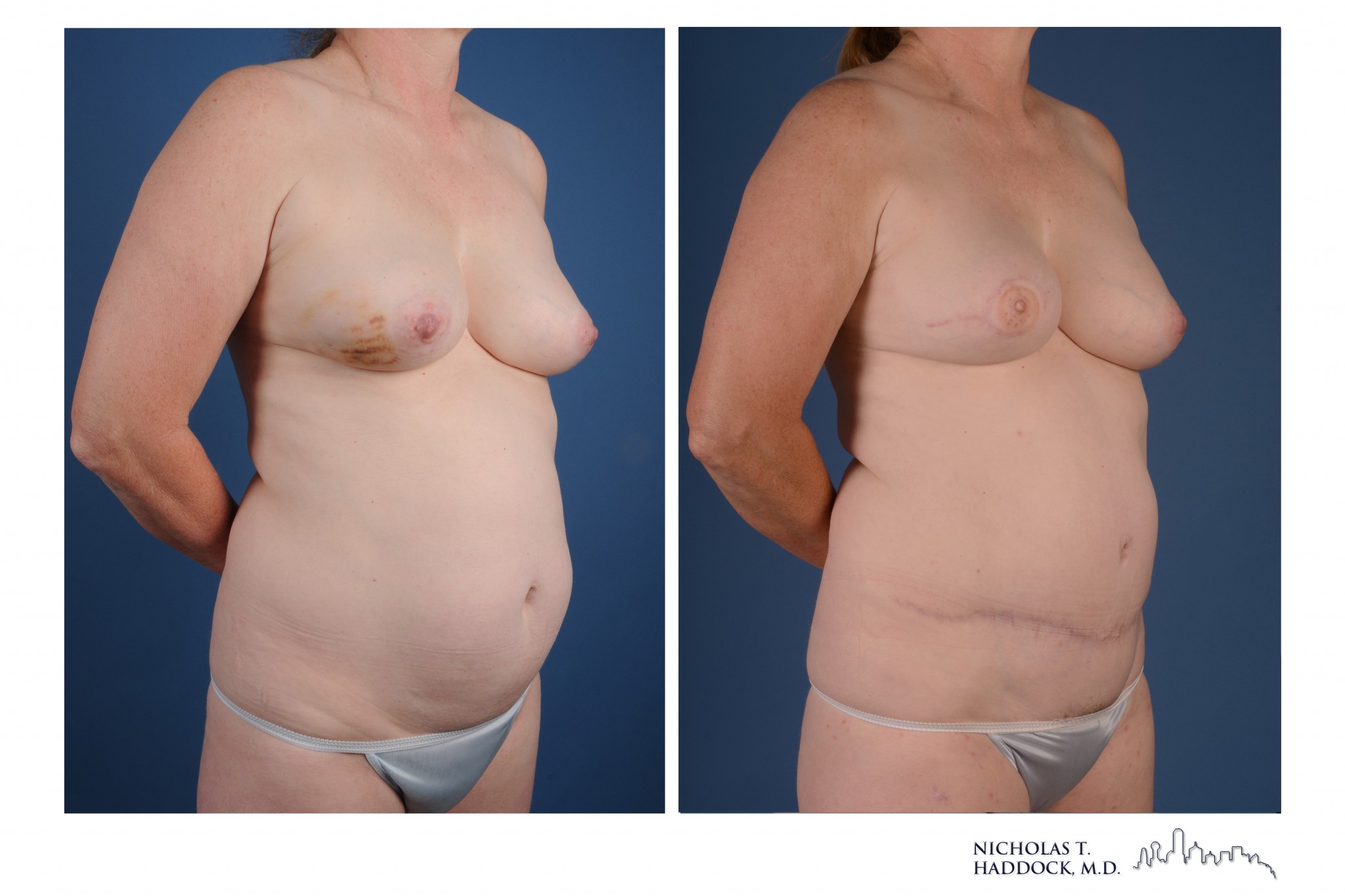

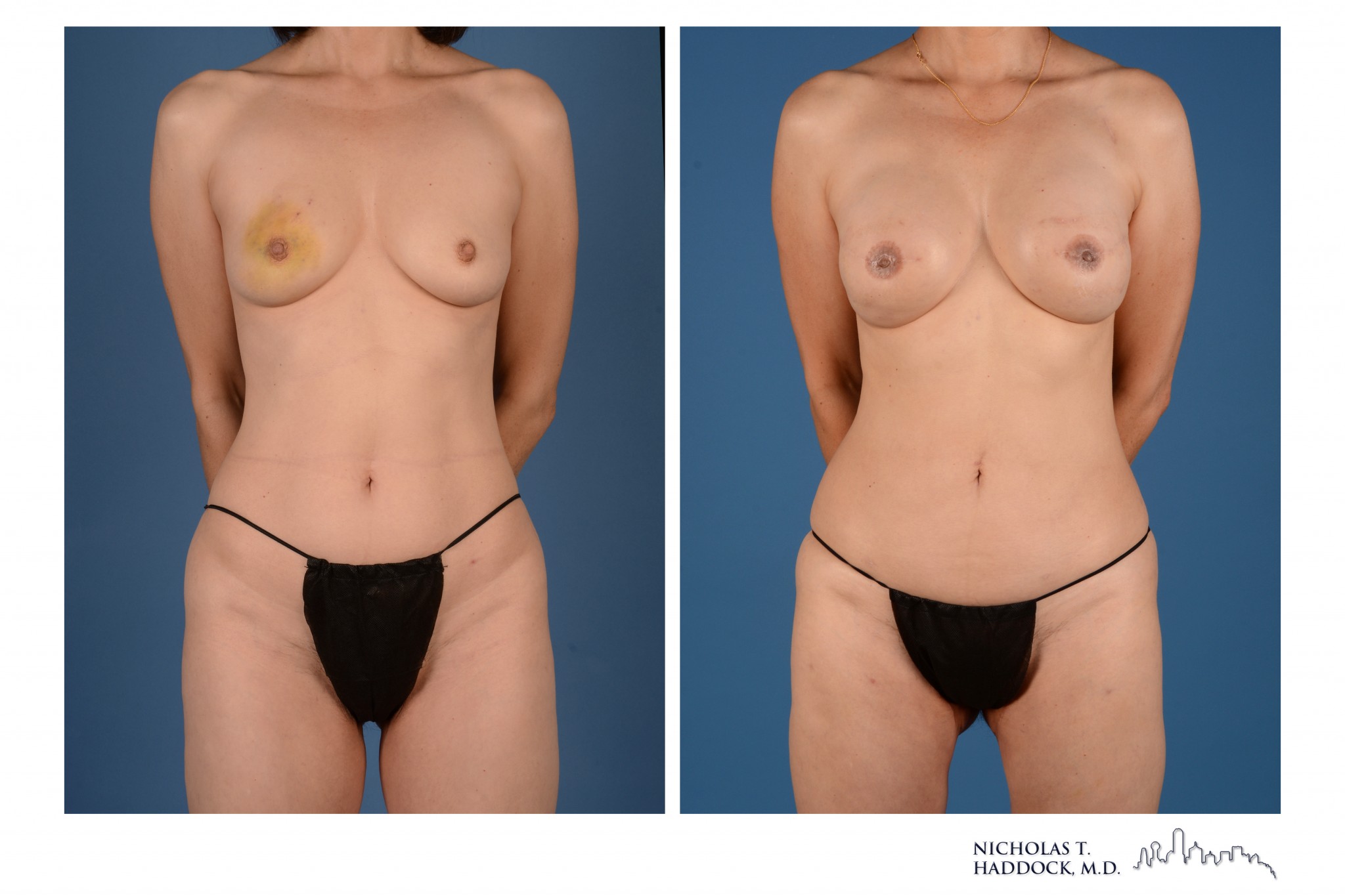
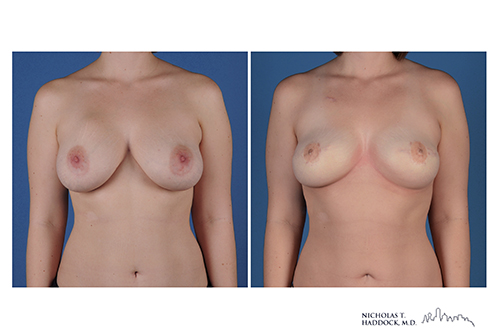
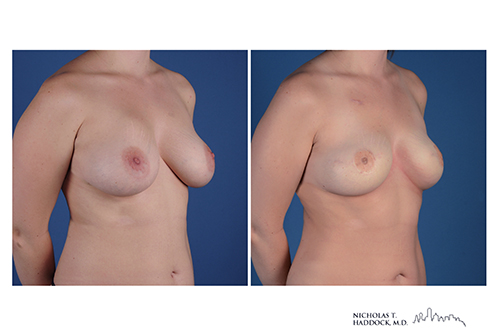
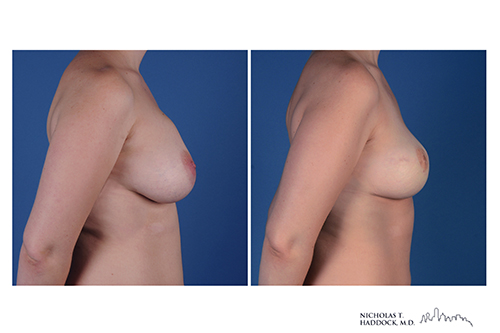
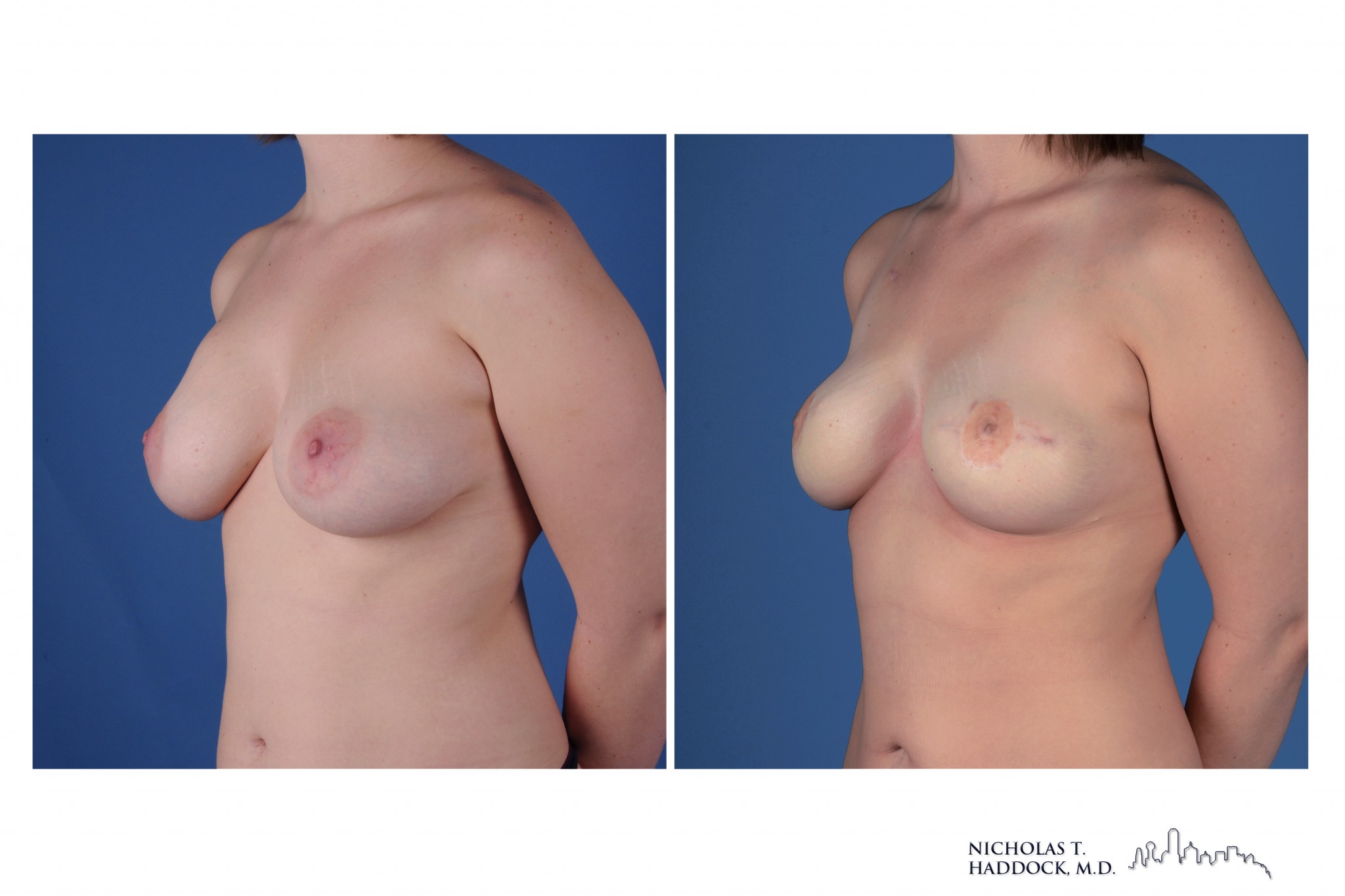
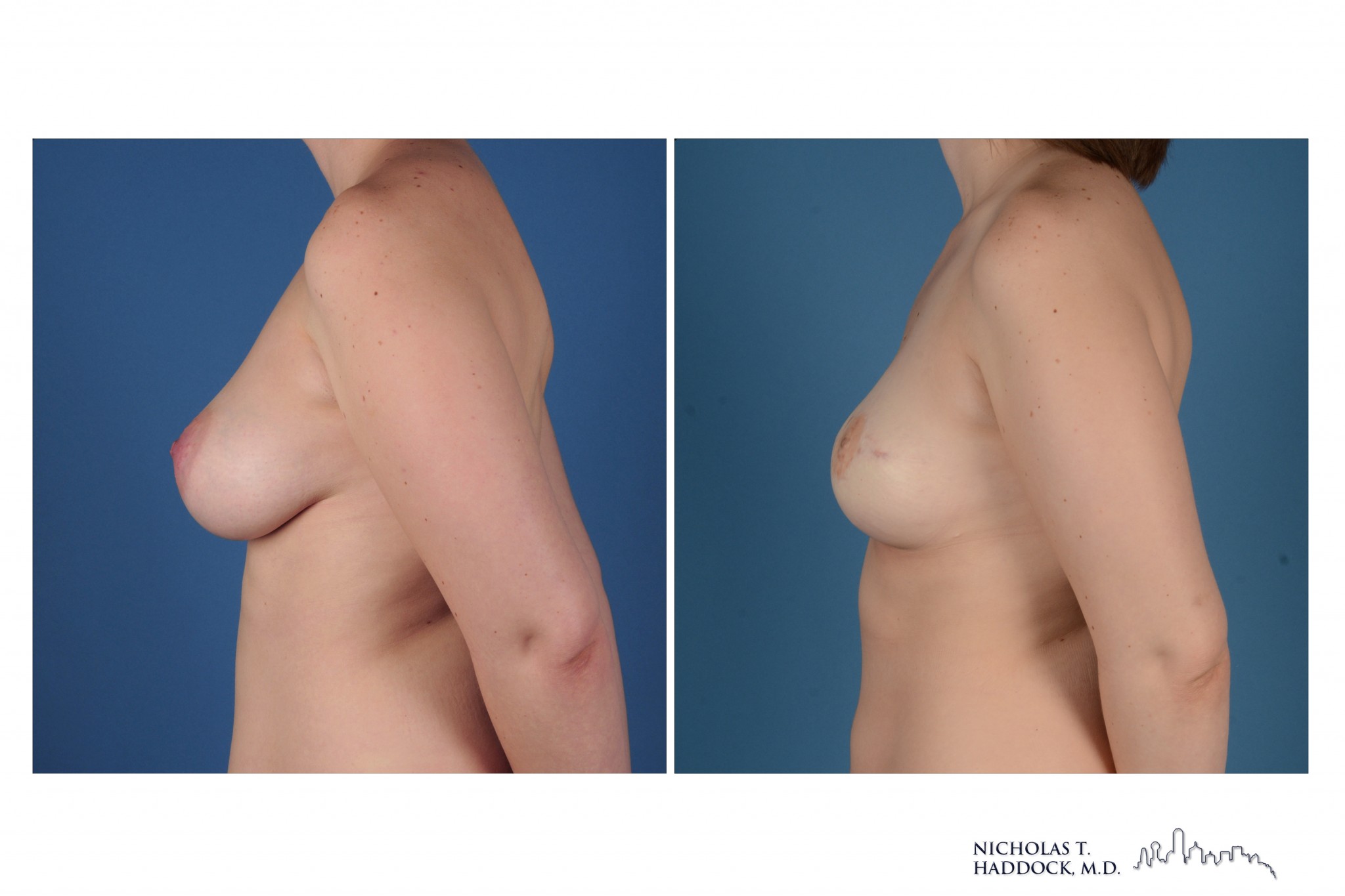
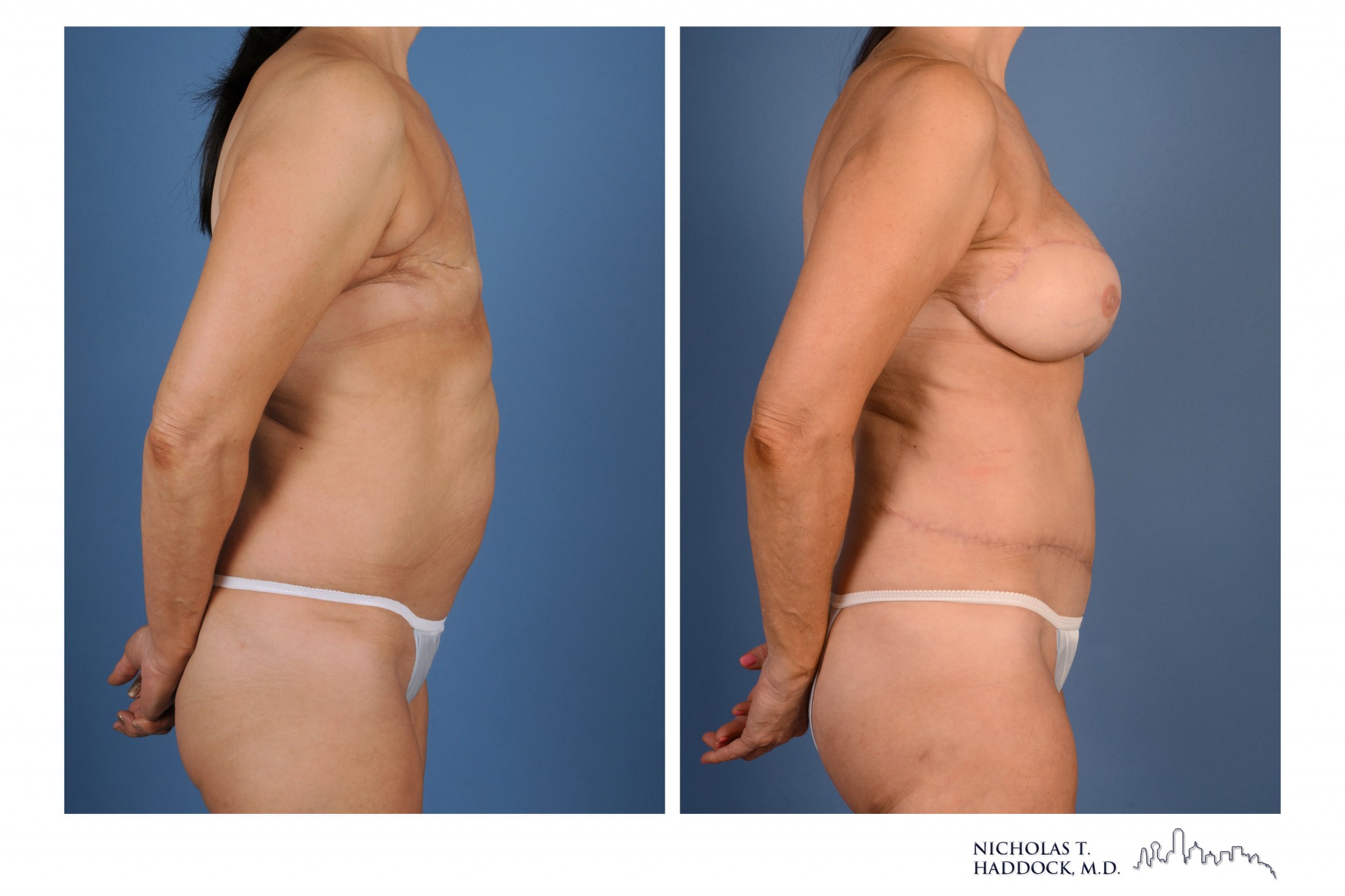
Right mastectomy followed by right DIEP flap and nipple reconstruction

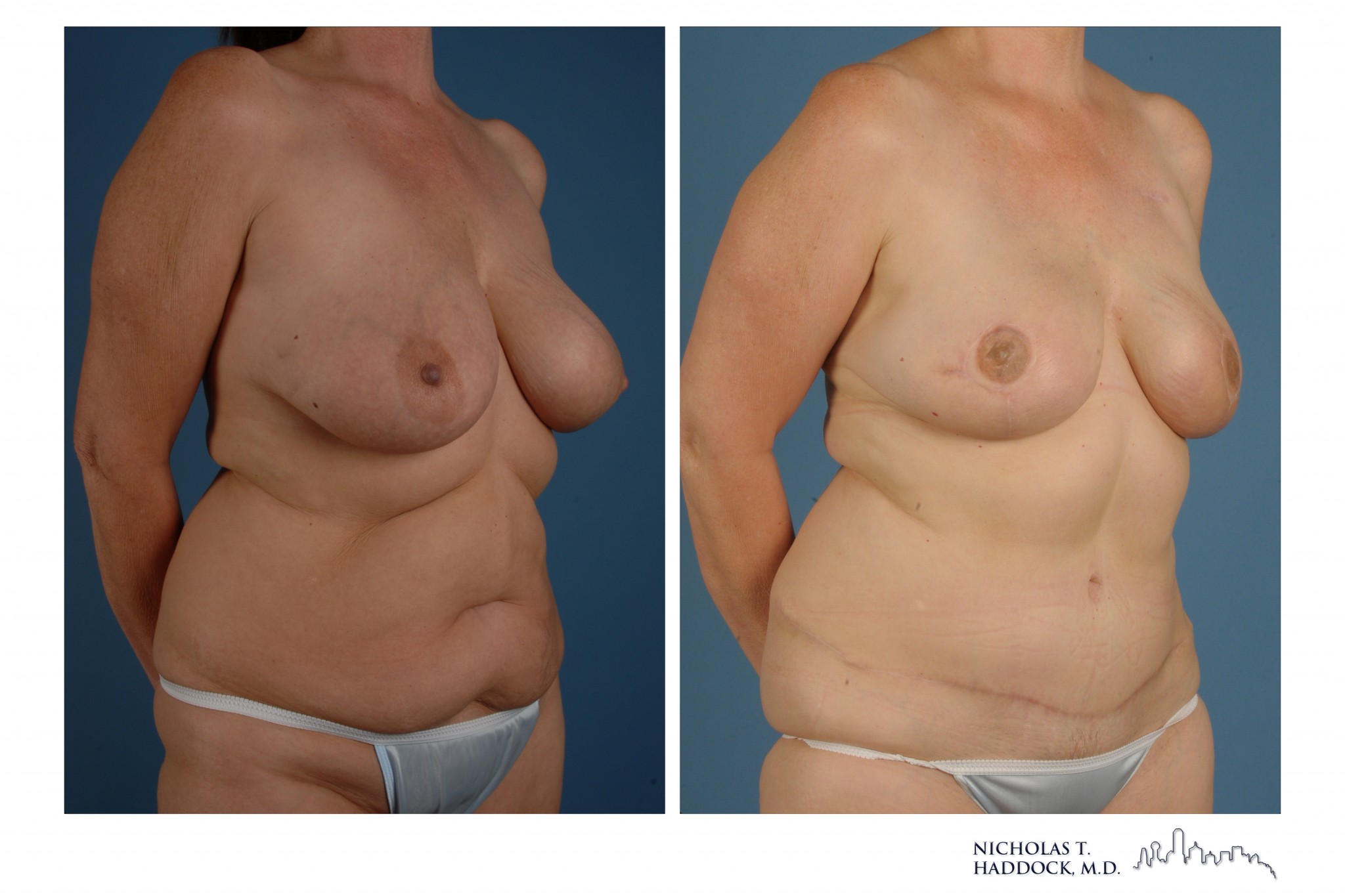

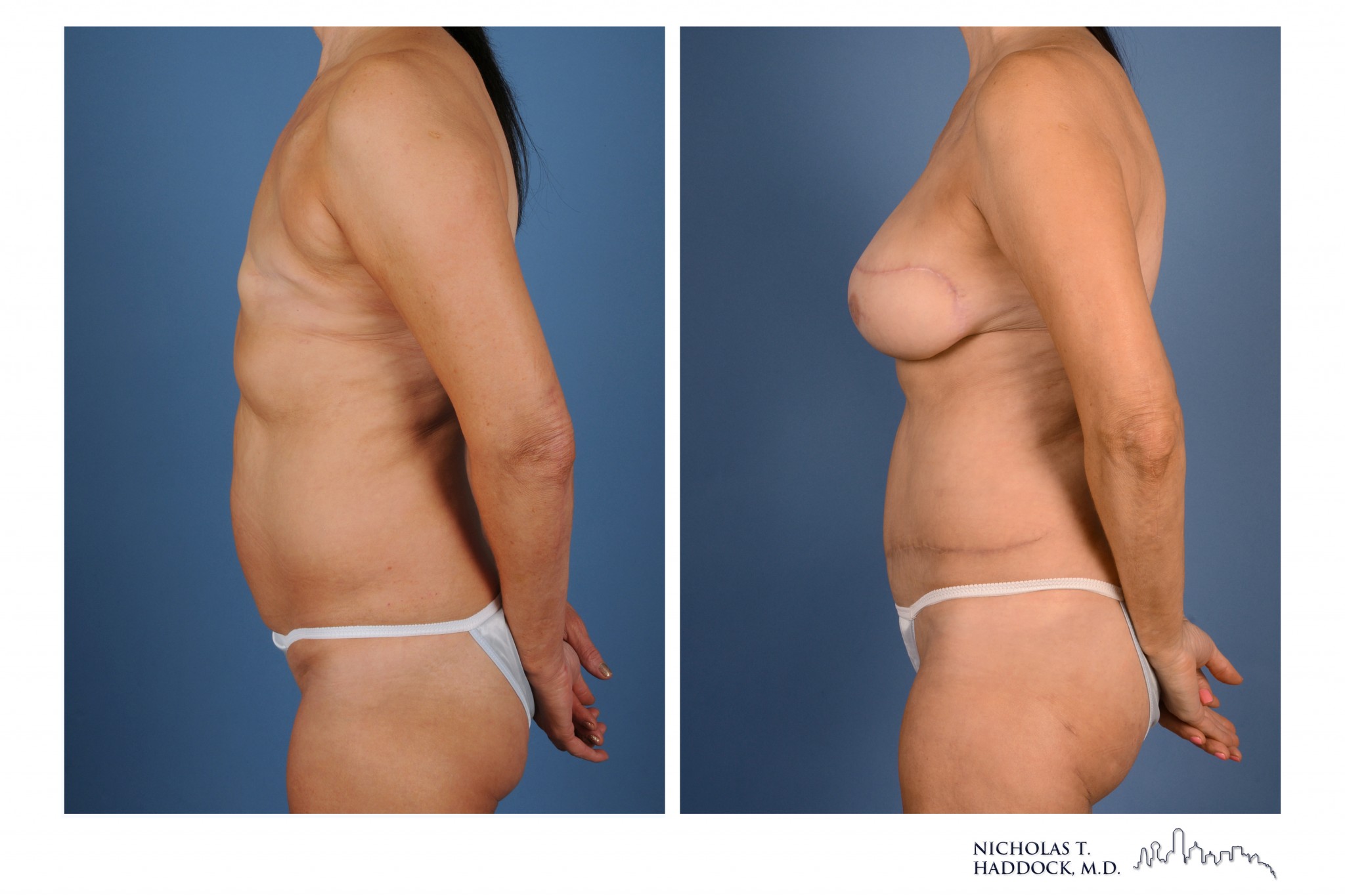
Bilateral mastectomies followed by bilateral DIEP flaps and nipple reconstruction
PAP Flap
The Profunda Artery Perforator (PAP) flap is an excellent donor site option for women who have had previous abdominal surgery or have limited abdominal tissue. The PAP flap utilizes the tissue of the posterior thigh. The scar of the PAP flap can often be well hidden in the crease of the thigh and lower buttock. Other advantages of the PAP flap are that this area of the body contains rigorous and lengthy blood vessels that allow for versatility in choosing the positioning within the breast pocket. In addition to this, its elliptical design provides an ideal shape for coning to create a natural breast. Because the dissection avoids the inguinal lymphatics, there is also a potential reduction in the risk of lymphedema and seromas in comparison to other thigh flaps such as the TUG (transvers upper gracilis) flap. Like all other perforator flaps, the PAP flap transfers only the skin and fat, thereby leaving the muscle in place to preserve function.

Dr. Haddock is truly a world expert in the PAP flap. He has performed hundreds of these flaps with very high success rates. He was a co-author in the sentinel paper and has written multiple papers on this flap since the original. He often speaks on this topic at regional, national and even international meetings. Additionally, Dr. Haddock has one of the largest experiences in this flap in the country if not the world.
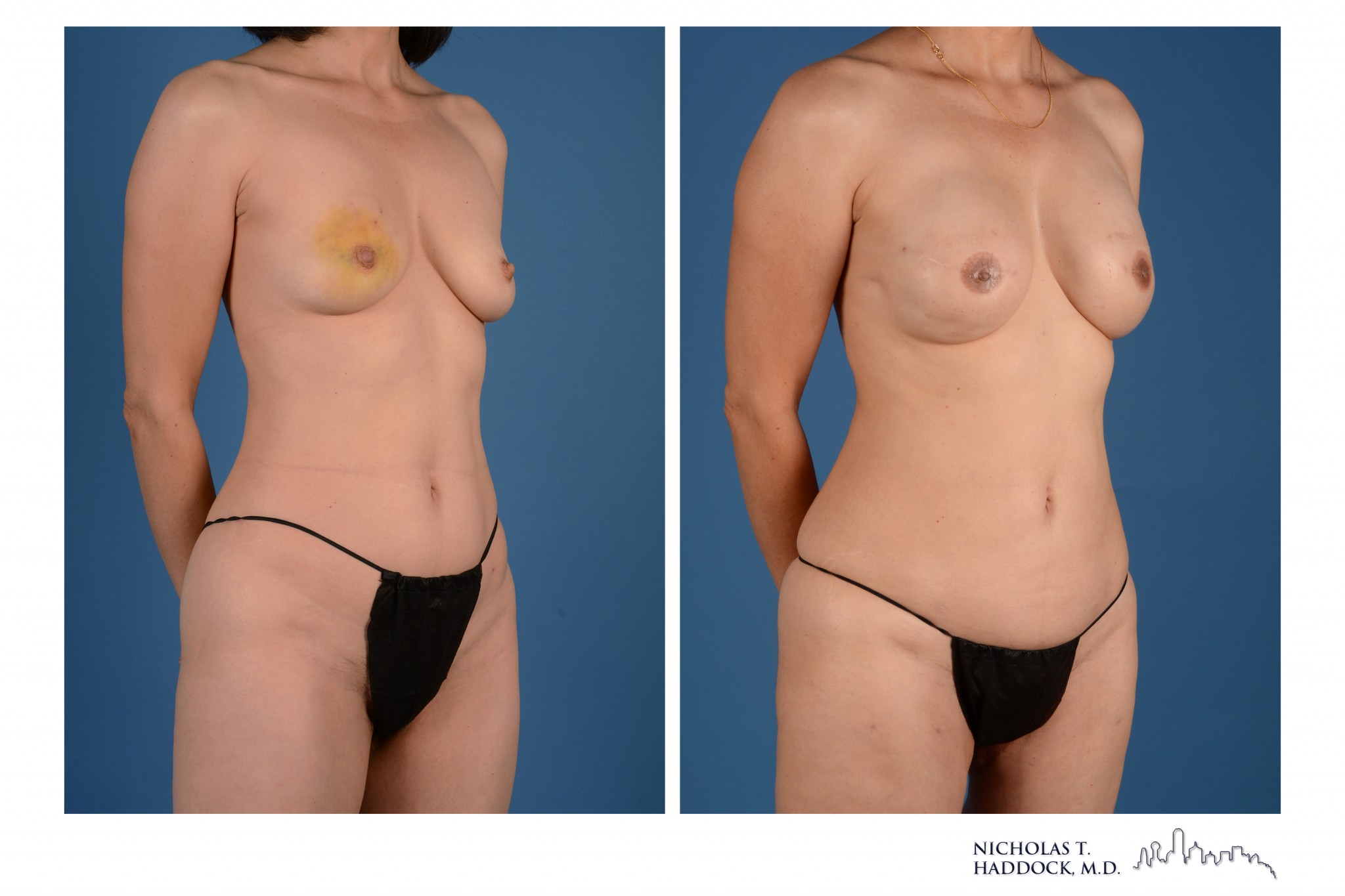
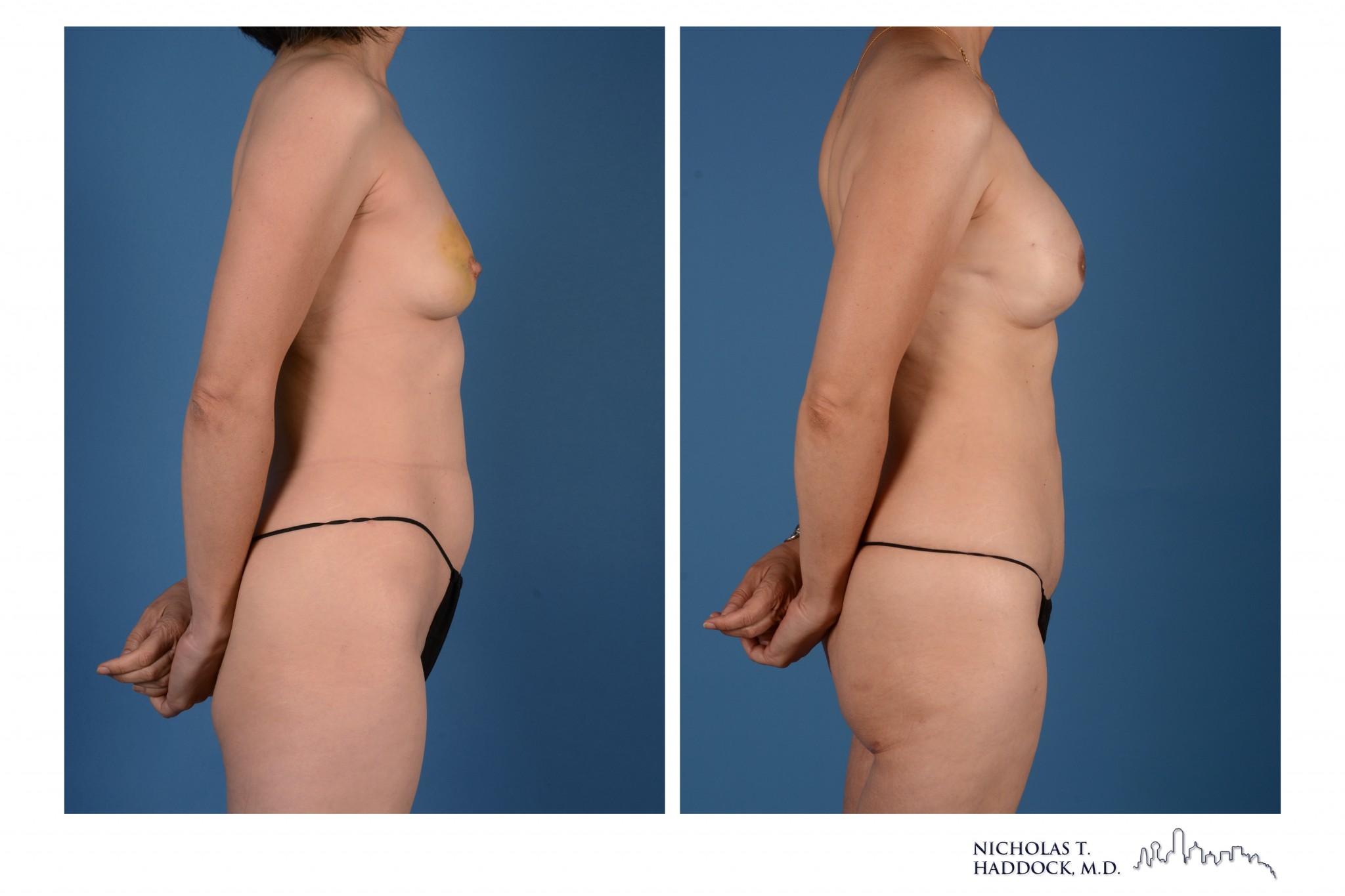
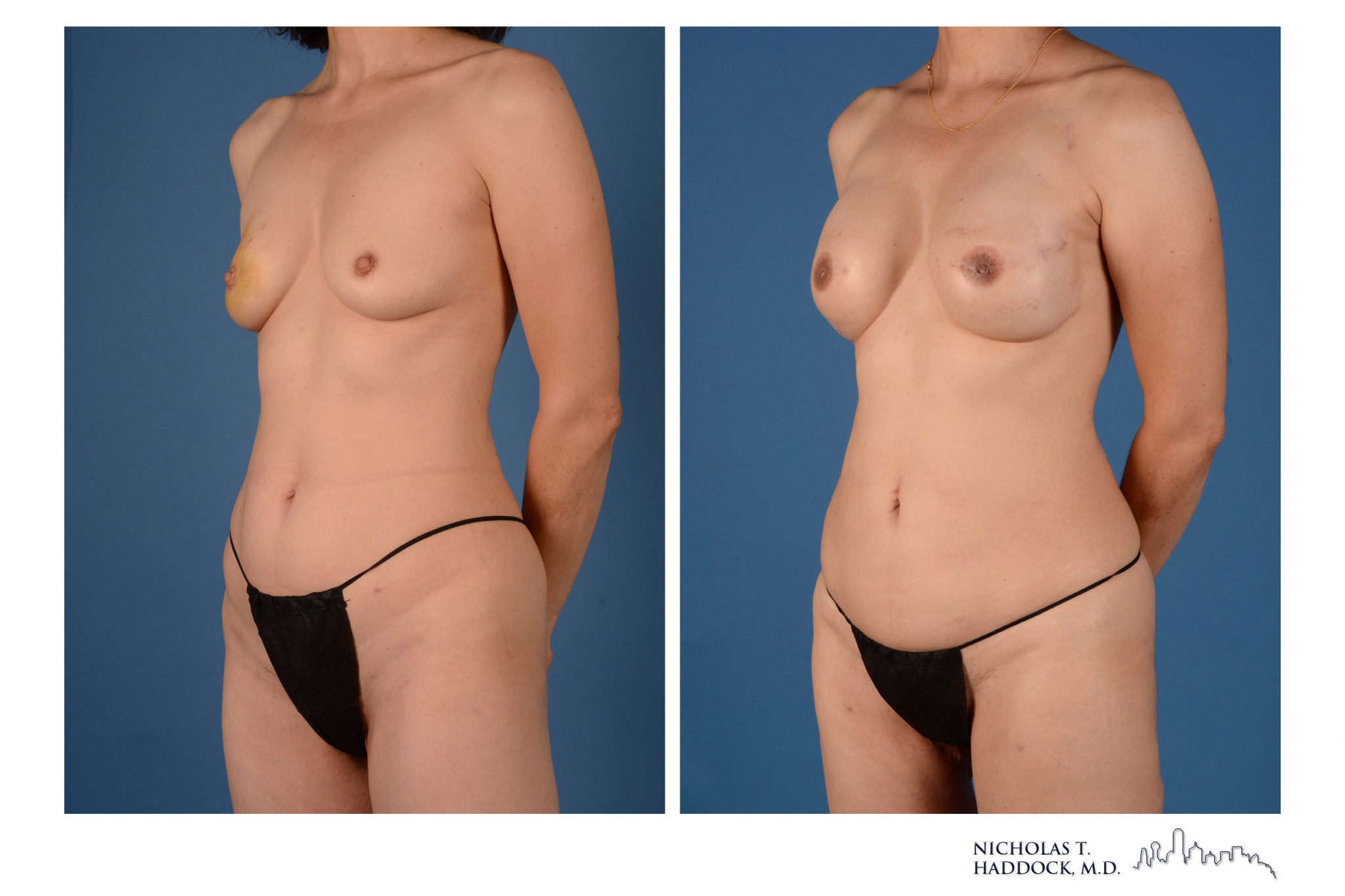


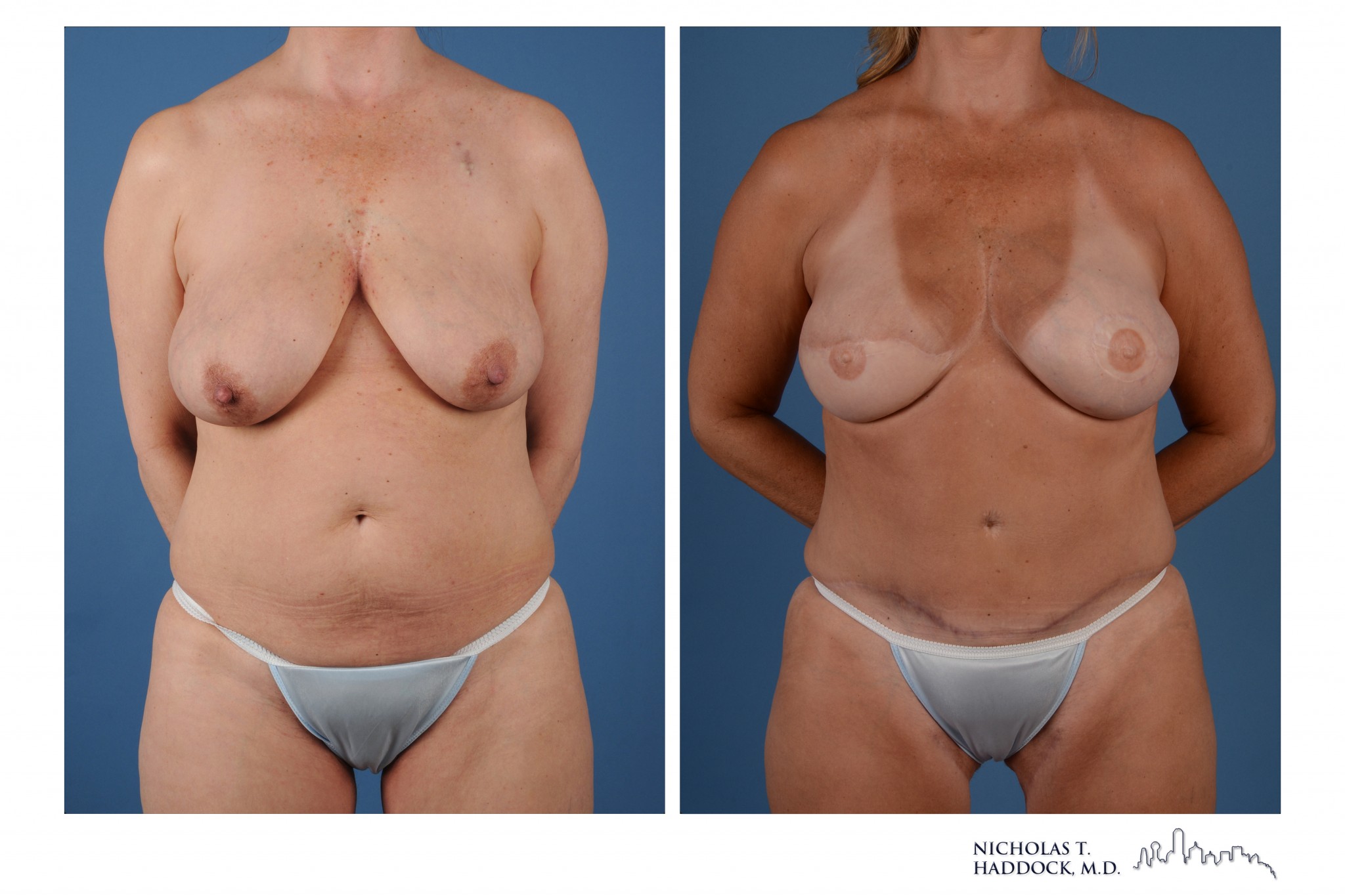
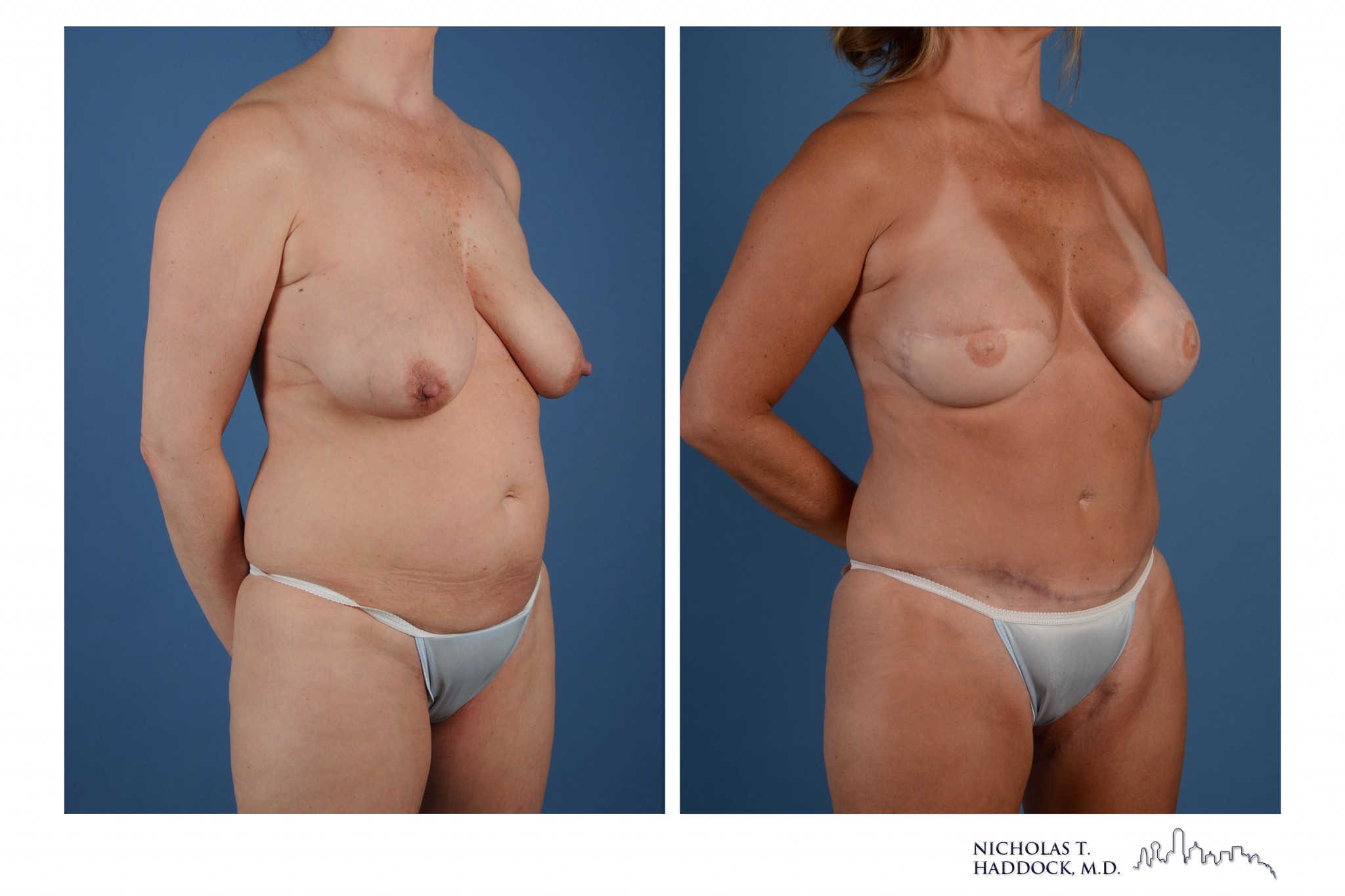
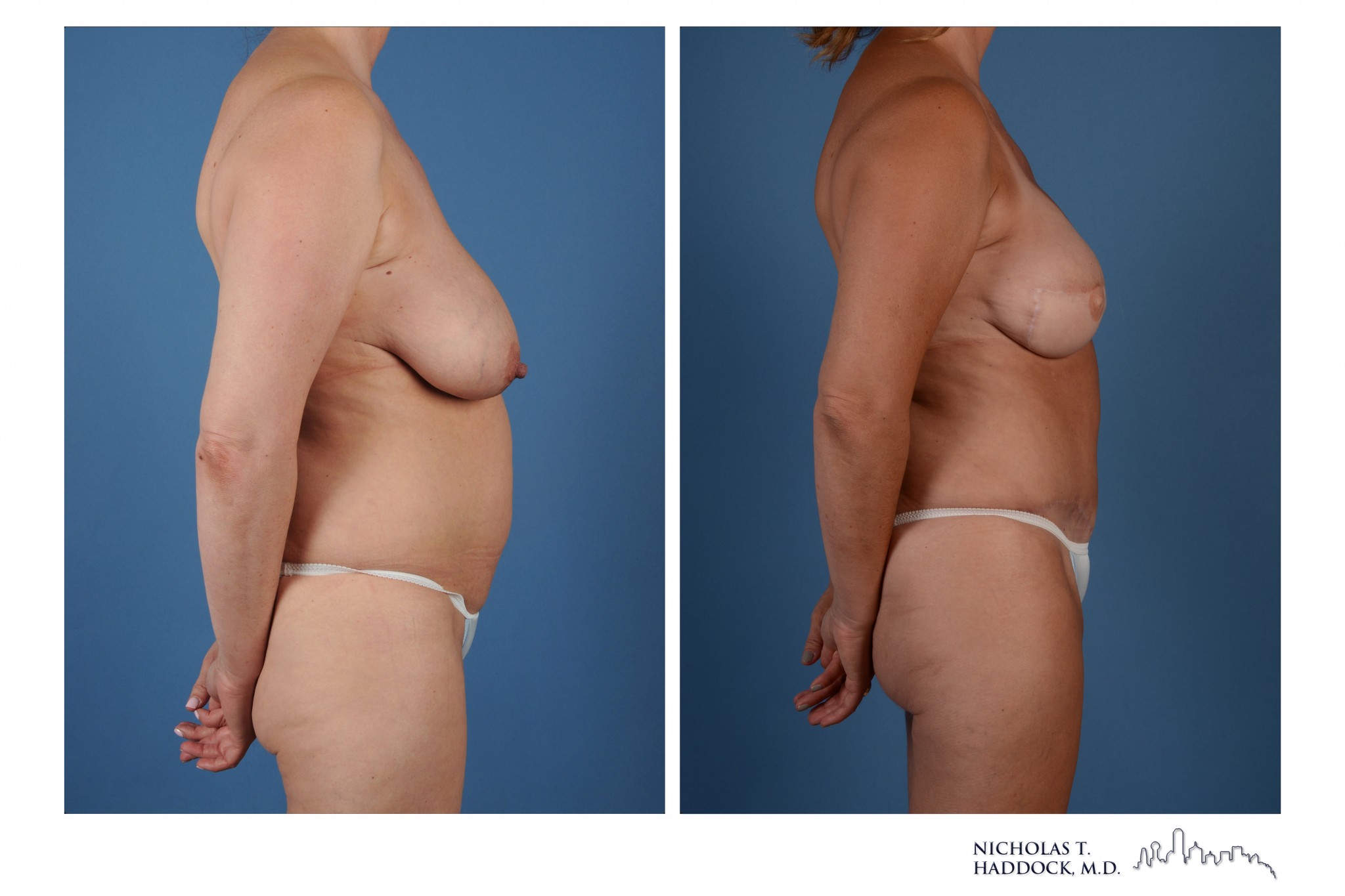
Bilateral mastectomies followed by bilateral PAP Flaps and nipple reconstruction
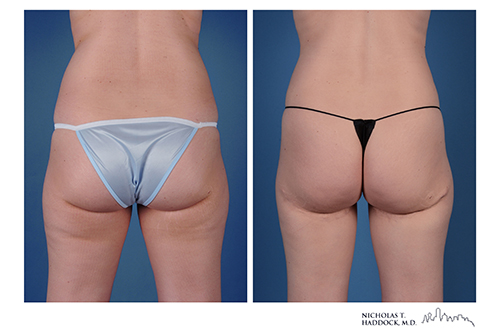
Bilateral mastectomies followed by bilateral PAP Flaps and nipple reconstruction
Dr. Haddock’s PAP Flap Publications

Versatility of the Profunda Artery Perforator Flap: Creative Uses in Breast Reconstruction
Dr. Haddock’s paper describing the first 73 PAP flaps done in Dallas Fort Worth. The PAP flap is a versatile flap for different types of breast reconstruction. visit the Plastic and Reconstructive Surgery Journal
Double Flaps or Stacked Flaps
Double flaps is when two flaps are used for one breast. The most common variant of this is a Double DIEP flap in which both sides of the abdomen are used for one breast reconstruction. Double PAPs can also be employed for patients that require unilateral breast reconstruction but one thigh is not sufficient. Dr. Haddock and his partner Dr. Teotia have one of the largest experiences with these types of procedures in the country. They have presented on this in local, regional and national meetings.
4 Flaps
The 4 flap breast reconstruction refers bilateral DIEP flaps and bilateral PAP flaps performed at the same time. This is a unique operation that is only employed in specific situations. In a subset of patients the abdomen or thigh alone will not provide enough tissue for total breast reconstruction. By using both the abdomen and the thighs as is done in the 4 flap breast reconstruction we can obtain adequate skin and volume to perform total breast reconstruction. In these complex situations using only one location would compromise the final aesthetic result. The use of multiple flaps avoids this compromise to the breast. Additionally it allows a more conservative surgery at the donor site ultimately limiting the morbidity of the thighs and abdomen.
Dr. Haddock performs these procedures with his partner Dr. Teotia. Together they are pioneers in this procedure and have one of the largest experiences with 4 flap breast reconstruction in the country.
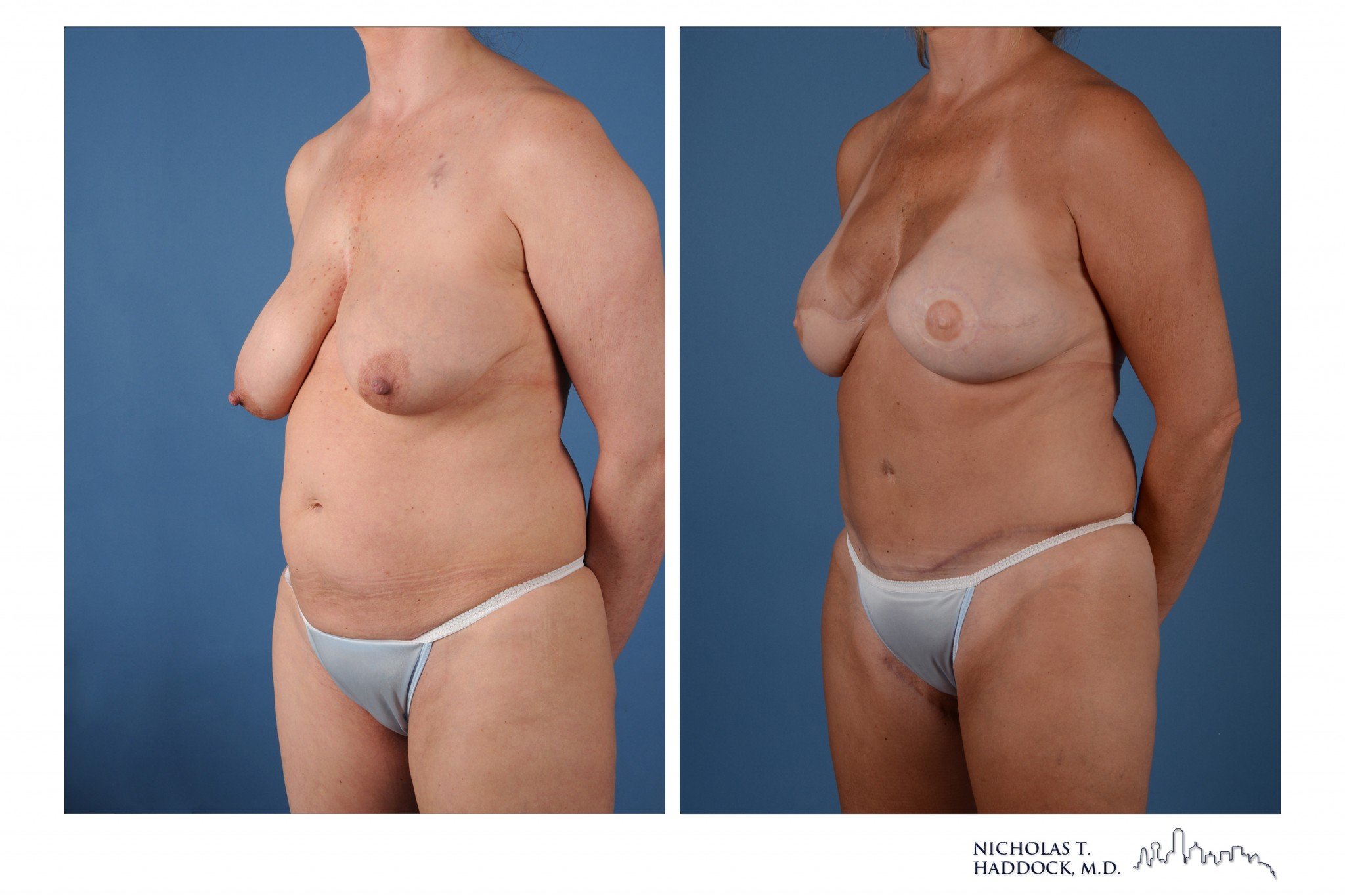
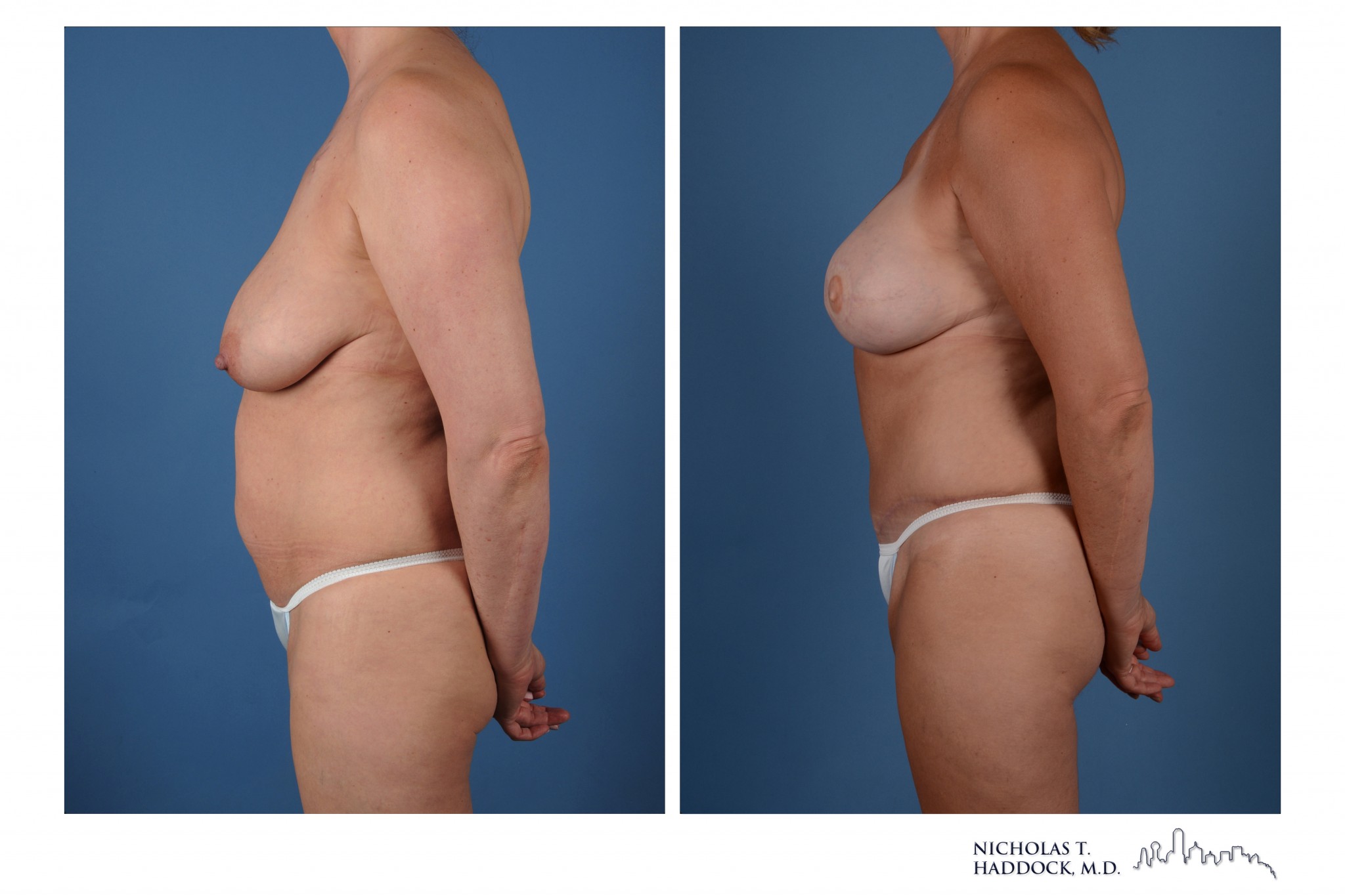

Bilateral mastectomies, right radiation, bilateral DIEP flaps and PAP flaps (4 Flap)
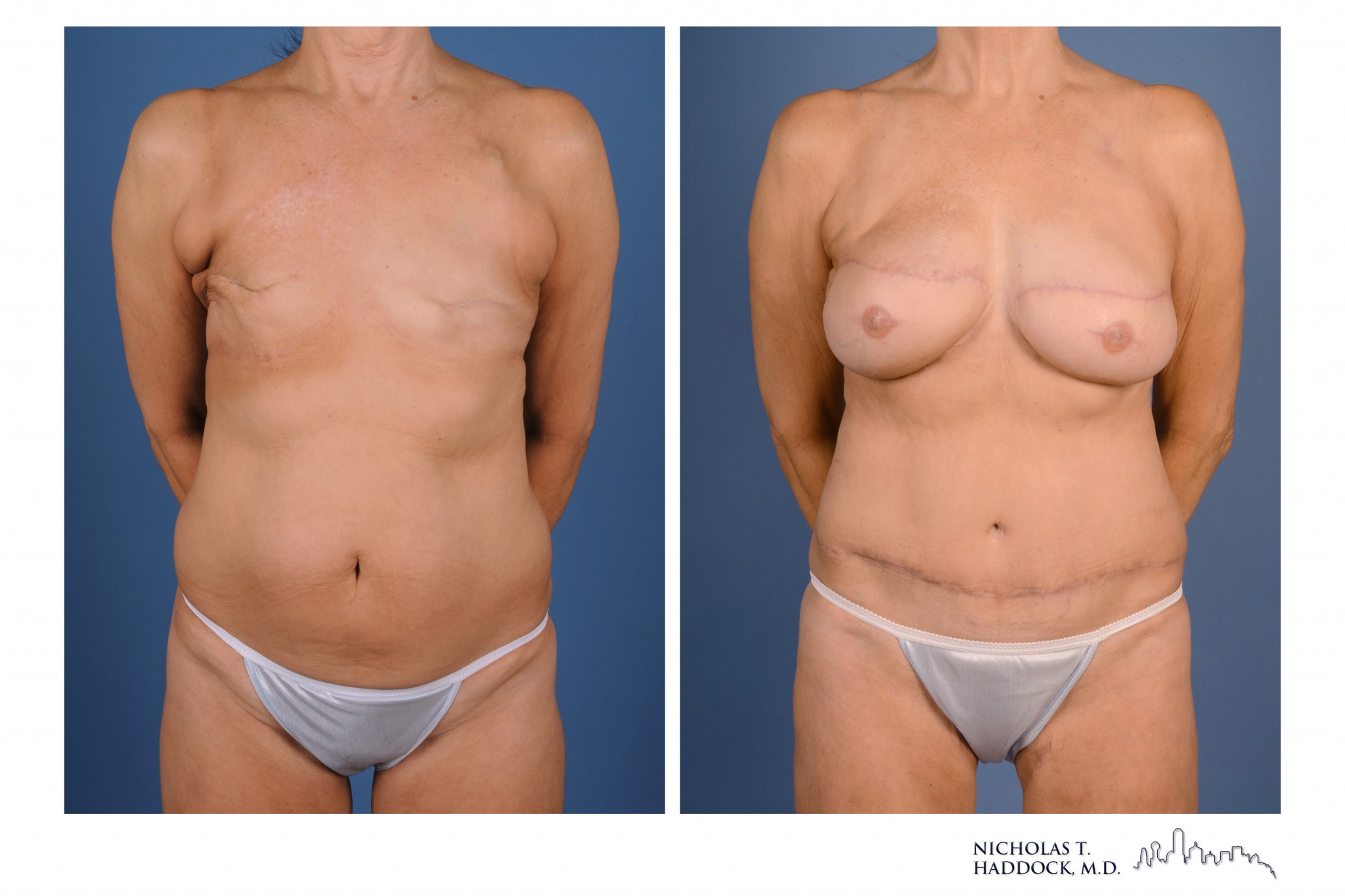
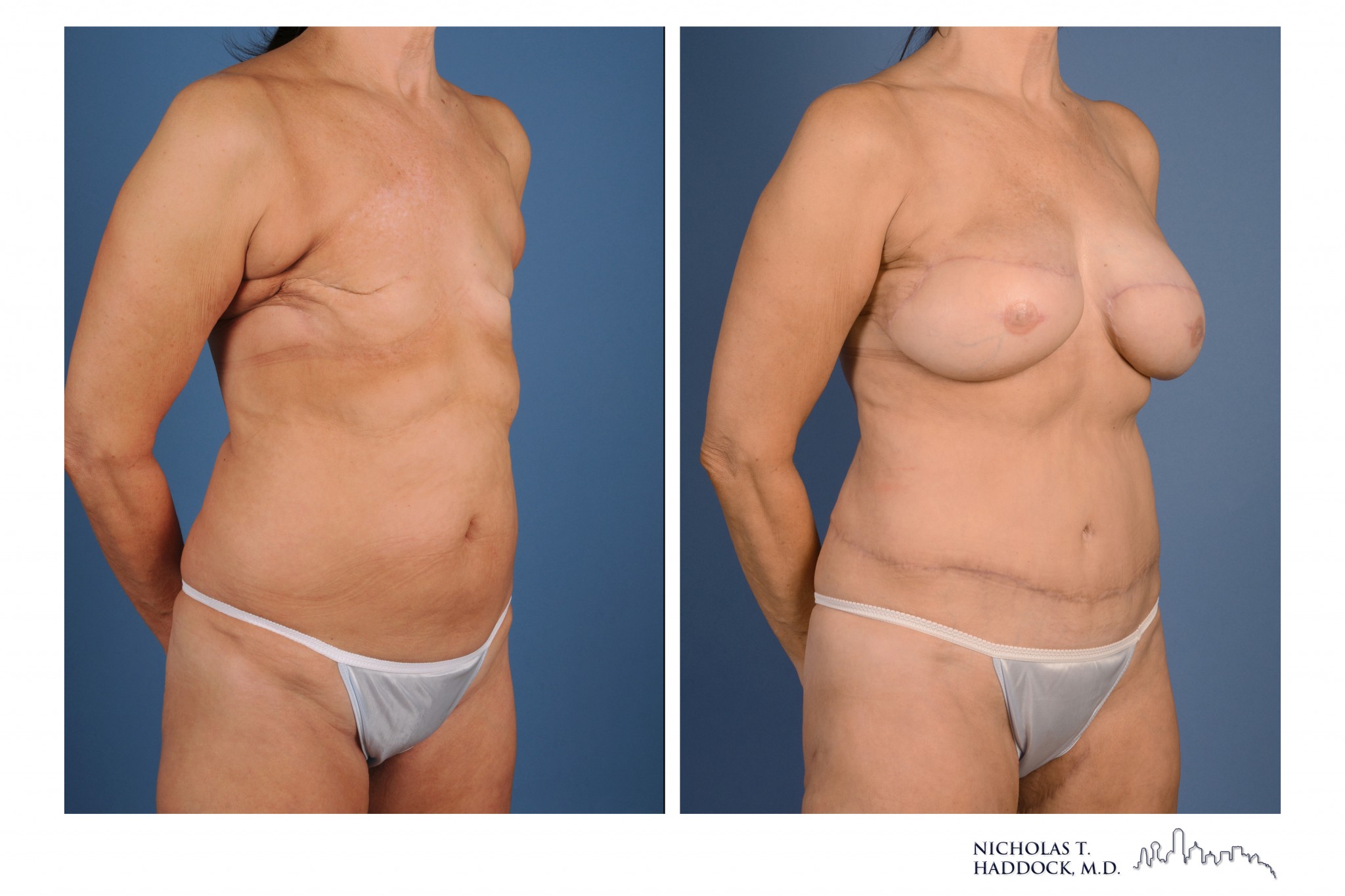


Bilateral mastectomies, right radiation, bilateral delayed DIEP flaps and PAP flaps (4 Flap)